Translate this page into:
Radiofrequency ablation of bilateral nevoid hyperkeratosis of nipple and areola
Correspondence Address:
Anupama Singh
M2/9, Shri Krishna Puri, Jaya Prakash Path, Patna - 800 001, Bihar
India
| How to cite this article: Singh A. Radiofrequency ablation of bilateral nevoid hyperkeratosis of nipple and areola. Indian J Dermatol Venereol Leprol 2016;82:730-732 |
Sir,
A 22-year-old unmarried woman had complaints of progressive darkening and irregular thickening of both nipples and areolae of about 7 years duration. It had become stable in the last 2 years. There was no itching, discharge or pain. Lesions were limited to nipples and areolae and were not present on other parts of the body. She was not obese or taking any hormonal treatment. Her medical and family history was unremarkable.
Examination showed diffuse hyperpigmented and hyperkeratotic verrucous papules coalescing to form plaques involving the entire nipple and areola on both sides, more pronounced on the right [Figure - 1] and [Figure - 2]. No underlying lump was palpable. There was no nipple discharge, retraction or lymphadenopathy. Complete blood counts and routine biochemical tests were normal. A sono-mammogram was also normal.
 |
| Figure 1: Hyperpigmented verrucous plaques involving nipple and areola bilaterally |
 |
| Figure 2: Left breast showing hyperpigmented, verrucous papules coalescing into plaque involving nipple and areola |
Histopathological examination of the lesion showed hyperkeratosis, irregular acanthosis and broad papillomatosis with fibrovascular cores [Figure - 3]. The clinical presentation and histopathology confirmed the diagnosis of nevoid hyperkeratosis of nipple and areola.
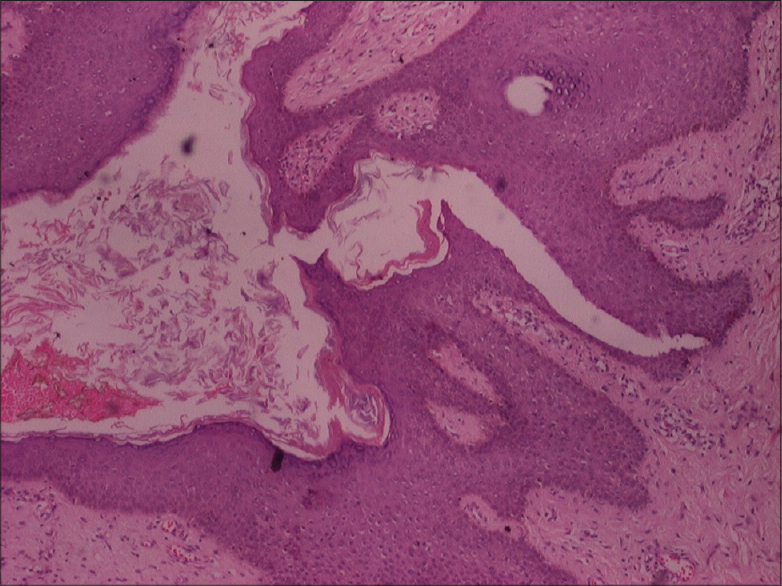 |
| Figure 3: There is hyperkeratosis, irregular acanthosis and broad papillomatosis with fi brovascular cores (H and E, ×40) |
The condition did not respond to 5 months of combination therapy with topical tretinoin and oral acitretin. Subsequently, radiofrequency ablation at half-maximal intensity was done in two sittings for each side. Lesions were removed tangentially in cutting mode with a circular loop. Care was taken to confine tissue destruction to the level of papillary dermis. As the bleeding was minimal, the operative field could be visualized clearly. Non-adherent antibiotic-impregnated dressing was used following ablation and a short course of oral antibiotics and analgesics were also given. The wound healed each time in 7–10 days with separation of a scab. Satisfactory cosmetic results were obtained in nipple and areola on both sides [Figure - 4] and [Figure - 5]. Post-ablation hypopigmentation occurred on one side but showed progressive improvement with time. No recurrence has been observed during one and half years of follow-up after the procedure.
 |
| Figure 4: Left breast 3 months following radiofrequency ablation |
 |
| Figure 5: Right breast 2 months following radiofrequency ablation |
Nevoid hyperkeratosis of nipple and areola is a rare, intriguing variant of hyperkeratosis of nipple and areola. The latter was first described by Tauber in 1923 as a benign dermatologic change in nipple and areola.[1] In 1938, Levy-Frankel subdivided hyperkeratosis of nipple and areola into three main types.[2] Type I shows hyperkeratosis of nipple and areola as an extension of epidermal nevus, type II shows hyperkeratosis of nipple and areola associated with other skin dermatoses such as atopic disease, acanthosis nigricans, ichthyosis, Darier's disease, seborrheic keratosis and Bowen's disease and type III is idiopathic or nevoid hyperkeratosis (nevoid hyperkeratosis of nipple and areola) and has no association with epidermal nevus or other dermatoses.
Our patient showed type III hyperkeratosis of nipple and areola (nevoid hyperkeratosis of nipple and areola). More than 50 cases have been reported in the literature;[3] we were able to find only four previous cases reported from India.[4],[5],[6]
The condition usually presents as a diagnostic dilemma due to its variable presentation and rarity. Unknown pathogenesis and rarity of the condition account for the lack of specific management guidelines. It predominantly affects women (approximately 80%) who generally present for the first time in the second to third decade.[3] In contrast, the age of onset in men is variable. Hyperpigmented, hyperkeratotic plaques of nipple and areola are the most characteristic presentation.[1] Lesions are usually bilateral, may involve nipple, areola or both and are asymptomatic, the primary concern being cosmetic. Difficulty in breastfeeding has been reported in some.
Type III (nevoid hyperkeratosis of nipple and areola) has to be differentiated from type I and type II hyperkeratosis of nipple and areola. Paget's disease, Bowen's disease, dermatophytosis and basal cell carcinoma are other differential diagnoses.
The etiology of nevoid hyperkeratosis of nipple and areola is unknown. Changing estrogen level is proposed to be a triggering factor, suggested by Mold and Jegasothy on the basis of two patients who the condition after receiving diethylstilbestrol therapy for adenocarcinoma. Presentation during puberty and pregnancy and the change from unilateral to bilateral involvement during pregnancy further substantiate this theory.
There are limited reports regarding treatment options.[2] Keratolytics are the most commonly used agents but are not always effective. Cryotherapy and carbon dioxide laser have also been effective. Topical retinoic acid and calcipotriol have been used in the past. Surgical resection with grafting has been tried but there is a risk of a circumlinear scar.[7] Radiofrequency ablation is a cheap and easily available therapy that has been employed for many benign dermatologic disorders and there are two reports of its use in nevoid hyperkeratosis of nipple and areola in the past with encouraging results.[6],[8] In contrast to cryotherapy and carbon dioxide laser, the desired depth of tissue destruction is achieved in a controlled manner and the operative field is better visualized due to minimal bleeding during the procedure.[8]
Acknowledgment
I would like to thank Dr. Anil Kumar Singh for reviewing the manuscript.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| 1. |
Baykal C, Büyükbabani N, Kavak A, Alper M. Nevoid hyperkeratosis of the nipple and areola: A distinct entity. J Am Acad Dermatol 2002;46:414-8.
[Google Scholar]
|
| 2. |
Levy-Frankel A. Ka les hyperkeratoses de l'areole et du mamelon. Paris Med1938;28:63-6.
[Google Scholar]
|
| 3. |
Krishnan RS, Angel TA, Roark TR, Hsu S. Nevoid hyperkeratosis of the nipple and/or areola: A report of two cases and a review of the literature. Int J Dermatol 2002;41:775-7.
[Google Scholar]
|
| 4. |
Chikhalkar SB, Misri R, Kharkar V. Nevoid hyperkeratosis of nipple: Nevoid or hormonal? Indian J Dermatol Venereol Leprol 2006;72:384-6.
[Google Scholar]
|
| 5. |
Shastry V, Betkerur J, Kushalappa PA. Unilateral nevoid hyperkeratosis of the nipple: A report of two cases. Indian J Dermatol Venereol Leprol 2006;72:303-5.
[Google Scholar]
|
| 6. |
Verma P, Pandhi D, Yadav P. Unilateral nevoid/primary hyperkeratosis of nipple and areola successfully treated with radiofrequency ablation. J Cutan Aesthet Surg 2011;4:214-5.
[Google Scholar]
|
| 7. |
Foustanos A, Panagiotopoulos K, Ahmad D, Konstantopoulos K. Surgical approach for nevoid hyperkeratosis of the areola. J Cutan Aesthet Surg 2012;5:40-2.
[Google Scholar]
|
| 8. |
Ozyazgan I, Kontas O, Ferahbas A. Treatment of nevoid hyperkeratosis of the nipple and areola using a radiofrequency surgical unit. Dermatol Surg 2005;31:703-5.
[Google Scholar]
|
Fulltext Views
1,643
PDF downloads
1,105





![[Figure - 1]](#fig_ijdvl_2016_82_6_730_186478_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2016_82_6_730_186478_f2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2016_82_6_730_186478_f3.jpg){kind=link}
![[Figure - 4]](#fig_ijdvl_2016_82_6_730_186478_f4.jpg){kind=link}
![[Figure - 5]](#fig_ijdvl_2016_82_6_730_186478_f5.jpg){kind=link}