Translate this page into:
Agminated lentiginosis or segmental neurofibromatosis: A diagnostic challenge
2 Department of Pathology, Faculty of Medicine, Menoufiya University, Shebin Elkoom 32817, Egypt
Correspondence Address:
Noha Mohammed Dawoud
Department of Dermatology, Andrology and STDs, Faculty of Medicine, Menoufiya University, Shebin Elkoom 32817
Egypt
| How to cite this article: Dawoud NM, Bakry OA, Dawoud MM, Samaka RM. Agminated lentiginosis or segmental neurofibromatosis: A diagnostic challenge. Indian J Dermatol Venereol Leprol 2016;82:75-77 |
Sir,
We present two cases with an unusual pattern of segmental spotty pigmentation that posed a diagnostic challenge.
A 16-year-old woman presented to the dermatology department with asymptomatic spotty brownish lesions that were present since early childhood and gradually increased in number over time. No history of excessive sun exposure was evident. Physical examination revealed numerous brown macules, unilaterally distributed on the right side of the neck extending to the right cheek and shoulder [Figure - 1].
 |
| Figure 1: Multiple lentigines localized on the right side of the neck and extending to the right shoulder (note the dermatomal distribution as shown in 1a) |
A 22-year-old woman was referred for evaluation of asymptomatic hyperpigmented spots on her lower abdomen that were present since birth and were progressively increasing in number and size with age. Examination revealed numerous pin-point light brown macules unilaterally distributed on the left groin and buttock extending upward to the lower abdomen and downward to the upper thigh. Four café-au-lait macules ranging in diameter from 1 to 4 cm were seen among brown spots. No neurofibromas could be detected [Figure - 2].
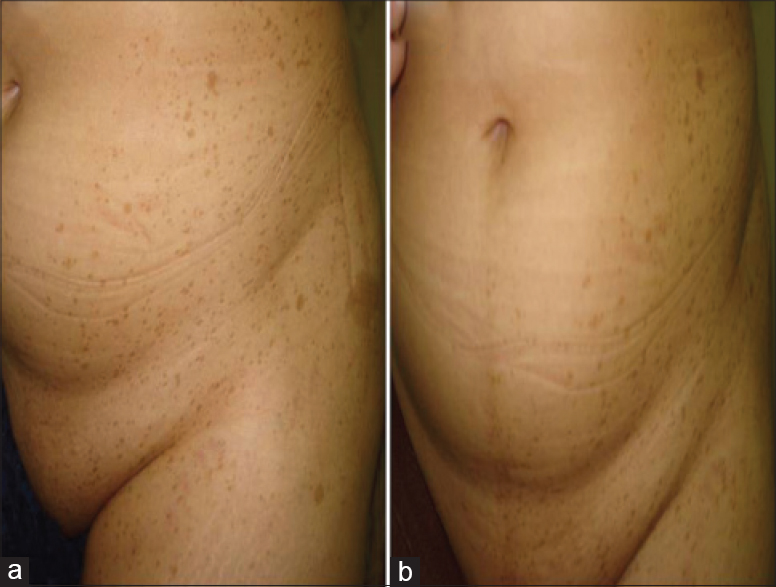 |
| Figure 2: (a) Multiple small, discrete, lightly pigmented macules together with four café-au-lait macules scattered over the left groin extending to the lower abdomen, buttock and upper thigh; (b) frontal view showing the segmental distribution of the pigmented macules with sharp demarcation at the midline |
In both the cases, physical and mental development was normal. Family history was non-contributory. No other cutaneous, mucosal or systemic findings were evident. Ophthalmic and orthopedic assessment revealed normal findings and routine laboratory investigations were within normal limits. Computed tomography and magnetic resonance imaging of the brain and spine revealed no abnormalities.
Histopathologic examination of skin biopsies from both cases revealed linear (non-nested) melanocytic hyperplasia in the epidermis with a hyperpigmented basal cell layer [Figure - 3]. In addition, the second case showed lentiginous elongation and thinning of the rete ridges [Figure - 3]b and [Figure - 3]c. Findings of both the cases were consistent with lentigo simplex. However, the biopsy taken from café-au-lait macules showed only increased melanin content of the basal cell layer.
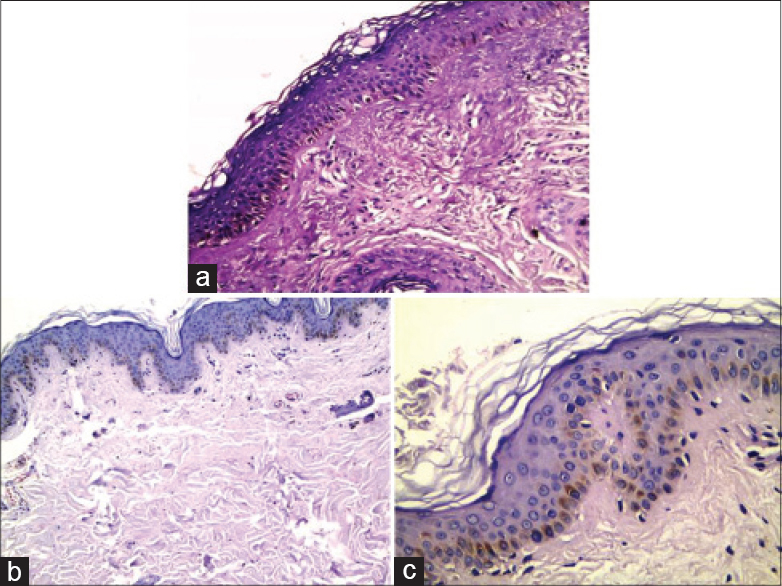 |
| Figure 3: (a) Case 1 lesion showing linear melanocytic hyperplasia in epidermis with hyperpigmented basal cell layer (H and E, ×200) (b) Case 2 lesion showing lentiginous hyperplasia of epidermal melanocytes with elongation and thinning of rete ridges (H and E, ×100), (c) Higher power view of the same lesion (case 2) with evident basal cell layer pigmentation (H and E, ×400) |
Based on both clinical and histopathologic criteria, our first case was diagnosed as agminated lentiginosis. However, in the second case, the presence of café-au-lait macules in the same segmental distribution represented a diagnostic problem. The question we faced was whether this was a case of agminated lentiginosis associated with café-au-lait macules as previously reported by some authors, 1 or whether it was segmental neurofibromatosis.
Agminated lentiginosis is a benign condition that is characterized by multiple lentigines that are grouped within an area of normal skin, often in a segmental pattern that can appear anywhere on the body. Differential diagnoses include speckled lentiginous nevus and segmental neurofibromatosis. Speckled lentiginous nevus was excluded in the present cases by the absence of a tan macular background and nevoid melanocytes on histopathology.[1]
Segmental neurofibromatosis is a rare condition characterized by pigmentary abnormalities which include café-au-lait macules and/or axillary freckles and/or neurofibromas in a single segment of the body that do not cross the midline. Family history of neurofibromatosis is not seen nor is systemic involvement. It is further subdivided into four subtypes: true segmental, localized with deep involvement, hereditary and bilateral.[2]
The presence of multiple café-au-lait macules in the same distribution as lentigines in cases of agminated lentiginosis has led some authors to suggest that it is a form of neurofibromatosis.[2] Chen et al. reported a case that confirmed that agminated lentiginosis represents a mosaic manifestation of neurofibromatosis 1.[3] Their case was had an unusual combination of multiple lentigines clustered on her left face, café-au-lait macules on her left arm with ipsilateral axillary freckling and Lisch nodules.
There are also reports of agminated lentiginosis in patients with either contralateral or bilateral segmental neurofibromatosis.[2] The diagnosis of segmental neurofibromatosis was based on both neurofibromas and café-au-lait macules in a segmental distribution or combined with Lisch nodules or scoliosis affecting the same side of the body and/or progeny who had classic neurofibromatosis.[1]
In our second patient, the absence of any associated manifestations of neurofibromatosis and the lentiginous hyperplasia revealed by histopathologic examination weighed more towards the diagnosis of agminated lentiginosis. However, in view of the contention that agminated lentiginosis might represent a forme fruste of neurofibromatosis or even be part of the spectrum of segmental neurofibromatosis,[4] the patient has to be followed up for any cutaneous or ocular lesions that may develop later on. The age of presentation of neurofibromas is from puberty to young adulthood but may occur at any age. Also, the presence of Lisch nodules is age-dependent; only 40% of affected children have them by 6 years of age, whereas by late adulthood, more than 95% of people with neurofibromatosis 1 will have Lisch nodules.[5]
In conclusion, the presence of café-au-lait macules does not confirm the diagnosis of segmental neurofibromatosis. Thorough history taking, examination, histopathologic evaluation and follow-up are mandatory to help in careful differentiation and exclusion. Whether they represent the association of two disorders or agminated lentiginosis represents the forme fruste of neurofibromatosis 1 needs to be settled by genetic studies (mutational analysis).
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| 1. |
Lee JH, Kim SE, Park K, Son SJ, Song KY. A case of agminated lentiginosis with multiple café-au-lait macules. Clin Exp Dermatol 2007;32:658-60.
[Google Scholar]
|
| 2. |
Roth RR, Martines R, James WD. Segmental neurofibromatosis. Arch Dermatol 1987;123:917-20.
[Google Scholar]
|
| 3. |
Chen W, Fan PC, Happle R. Partial unilateral lentiginosis with ipsilateral Lisch nodules and axillary freckling. Dermatology 2004;209:321-4.
[Google Scholar]
|
| 4. |
Kim HS, Kim SY, Kim GM. Extensive partial unilateral lentiginosis. J Eur Acad Dermatol Venereol 2006;20:469-70.
[Google Scholar]
|
| 5. |
Ruggieri M, Pavone P, Polizzi A, Di Pietro M, Scuderi A, Gabriele A, et al. Ophthalmological manifestations in segmental neurofibromatosis type 1. Br J Ophthalmol 2004;88:1429-33.
[Google Scholar]
|
Fulltext Views
8,755
PDF downloads
1,297





![[Figure - 1]](#fig_ijdvl_2016_82_1_75_171651_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2016_82_1_75_171651_f2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2016_82_1_75_171651_f3.jpg){kind=link}