Translate this page into:
Narrow band ultraviolet-B versus Goeckerman therapy for psoriasis with and without acitretin: A retrospective study
Correspondence Address:
Ercan �aliskan
Department of Dermatology, Gulhane School of Medicine, Etlik/Kecioren/Ankara 06018
Turkey
| How to cite this article: �aliskan E, Tunca M, A�ikg�z G, Arca E, Y�rekli A, Akar A. Narrow band ultraviolet-B versus Goeckerman therapy for psoriasis with and without acitretin: A retrospective study. Indian J Dermatol Venereol Leprol 2015;81:584-587 |
Abstract
Background: Narrow band ultraviolet-B (NB-UVB) is now one of the most widely used modalities in the treatment of psoriasis. However, despite its high efficacy, conventional Goeckerman treatment has fallen out of favor in recent years and some institutions are now using NBUVB with coal tar as their regimen. Objective: To evaluate the efficacy of NB-UVB, Goeckerman therapy and the effect of addition of retinoid to the treatment regimen in the treatment of psoriasis,. Patients and Methods: A retrospective analysis of 65 patients who underwent 81 courses of treatment in our department was undertaken. The efficacy of NB-UVB and Goeckerman therapy individually, and in combination with acitretin was assessed. Data were analysed to evaluate the contribution of acitretin to these modalities. Results: PASI-75 responses in the NB-UVB, retinoid + NB-UVB (re-NB), Goeckerman and retinoid + Goeckerman (re-Goeckerman) groups were achieved for 12 of 31 patients (39%), 13 of 21 patients (62%), 15 of 17 patients (88%) and 10 of 12 patients, respectively. The addition of acitretin to both modalities reduced both the number of sessions and the cumulative ultraviolet-B dose delivered. Limitations: This is a retrospective study, the patients were not randomized and the number of patients in the treatment groups were dissimilar. Conclusion: Goeckerman therapy is more effective than NB-UVB phototherapy. Although the addition of acitretin to both NB-UVB and Goeckerman therapy did not contribute to treatment outcomes in terms of PASI-75 responses, it enabled a reduction in UV exposures and enhanced efficacy.Introduction
NB-UVB is now the first choice among phototherapy options while Goeckerman treatment has fallen out of favour in recent years. However, the latter is still used in many dermatology clinics even in the age of biologics.[1],[2] Despite its many disadvantages (it is cumbersome, messy, time consuming and hospital based), Goeckerman therapy is stated to be at least comparable to biologics in terms of efficacy and time to response. A recent study of psoriasis treated by Goeckerman therapy by Lee and Koo found PASI-75 response rates of 56%, 96% and 100% at the end of 4, 8 and 12 weeks respectively, and they stated that none of the currently available treatment options for psoriasis could achieve the effectiveness of Goeckerman therapy from the standpoints of speed (56% at 4 weeks) and overall success (100% at 12 weeks).[3] Serrao and Davis evaluated the efficacy of Goeckerman therapy in 23 patients with psoriasis who were resistant to one or more biologic agents and achieved more than 80% clearance of psoriatic lesions in 87% of patients in an average duration of 23 days.[4]
A number of studies have evaluated phototherapy and its combinations with other modalities. Acitretin has been used in combination with NB-UVB phototherapy and Goeckerman therapy and the combinations were found to be more efficacious than monotherapy with NB-UVB and Goeckerman therapy.[3],[5],[6],[7],[8] However, there are only a few studies directly comparing NB-UVB with NB-UVB in combination with retinoid, and none of retinoids with Goeckerman therapy.
In this study, we retrospectively analyzed our data to compare the efficacy of Goeckerman therapy and NB-UVB and to evaluate if adding acitretin to these protocols contributed to treatment efficacy.
Patients and Methods
Study design
The study was approved by the local ethics committee. The data of patients treated between 2012 and May 2014 in our department (Gülhane Military Medical Academy, Department of Dermatology, Ankara, Turkey) were analyzed. Clinical data were obtained from inpatient and outpatient follow-up documents and matched with phototherapy records. After excluding the patients whose medical records were incomplete, 81 treatment periods in 65 patients were included in our analysis.
Treatment protocol
Routine laboratory examination was performed as part of the clinical protocol for phototherapy. Keratolytic salicylic acid ointments (5% to 10%) were given if indicated before the first phototherapy session. In patients who underwent Goeckerman therapy, a lotion containing 5% coal tar and 2% salicylic acid was used overnight followed by exposure to broadband ultraviolet-B (UVB) phototherapy in the morning, 5 days a week. The initial dosage of UVB was determined according to the Fitzpatrick skin type (between 20 and 40 mj/cm 2) and dosage increments are adjusted daily (usually 10–30 mj/cm 2) depending on the erythema response. In patients who were administered NB-UVB phototherapy, irradiation was performed 3 times a week and increased by 20% at each session.
In those patients in whom acitretin was administered, it was started as monotherapy for the first 2 weeks (10–35 mg/day) and then phototherapy was added. If acitretin was added to ongoing phototherapy sessions, the UV dosage was reduced by half. For all patients treated either with phototherapy alone or in combination with systemic treatments, topical agents (corticosteroids, salicylic acid, calcipotriol and combinations) were used for limited special areas (e.g., face, hands, etc.).
Evaluation of treatment outcomes
The response to treatment was assessed using psoriasis area and severity index (PASI) score. Less than 50% improvement in the PASI score relative to the baseline (<PASI-50) was classified “unresponsive” and more than 50% improvement (>PASI-50) as “responsive.” A “moderate response” was defined as 50–75% improvement and a “good response” as more than 75% improvement in PASI scores. Treatment outcomes depending on PASI-50 and PASI-75 responses, average numbers of treatment sessions and average cumulative UV dosages were evaluated. Topical treatments in combination with the phototherapy modalities were not taken into consideration.
Statistical analysis
Statistical analysis was performed on an SPSS 15.0 software package (SPSS Inc., Chicago, IL, USA) for Windows. The Kruskal–Wallis test was used for continuous variables and the Mann–Whitney U-test with Bonferroni correction was used for post-hoc test analyses. For non-contiguous variables the Chi-square test was performed and P < 0.05 was considered to be statistically significant.
Results
Sixty five patients who underwent a total of 81 courses of treatment (50 patients received single, 14 patients received two and one patient received three courses of treatment) were analyzed. NB-UVB was used in 52 of the courses (31 NB-UVB alone, 21 NB-UVB + acitretin) and the remaining 29 courses were of Goeckerman therapy (17 Goeckerman only, 12 Goeckerman + acitretin).
The treatment groups [Table - 1] were statistically similar (P > 0.05) in terms of age, duration of disease and gender. Initial PASI scores of the groups (mean ± standard deviation [SD]) were 11.1 ± 3.6, 12.9 ± 4.9, 13.2 ± 2.5 and 14.6 ± 4.0 in NB-UVB, re-NB-UVB, Goeckerman and re-Goeckerman groups respectively. A statistically significant difference was noted only between the NB-UVB and the re-Goeckerman group (P = 0.021).

The treatment responses are shown in [Table - 2]. All treatments were effective and a majority of the patients in each group achieved a PASI-50 response. Only 2 patients in the NB-UVB group, 1 patient in each of the three other groups were unresponsive (i.e., could not achieve PASI-50). There were no statistically significant differences in the PASI-50 response rates between the groups.
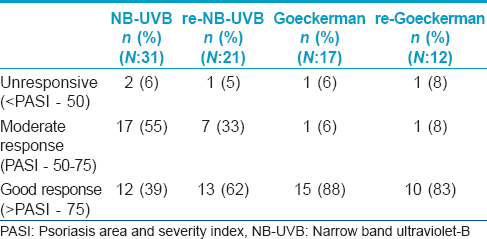
PASI-75 responses at the end of the phototherapy sessions [Table - 2] were achieved in 39% in the NB-UVB group, 62% in the re-NB-UVB group, 88% in the Goeckerman group and 83% in the re-Goeckerman group. A statistically significant difference between Goeckerman therapy groups and NB-UVB group was noted, but not the re-NB-UVB group. Although not statistically significant, a higher percentage of patients in the re-NB-UVB group achieved PASI-75 responses compared to the patients receiving NB-UVB alone (62% vs. 39%). Addition of acitretin to both NB-UVB and Goeckerman therapy did not contribute to treatment outcomes in terms of PASI-75 responses.
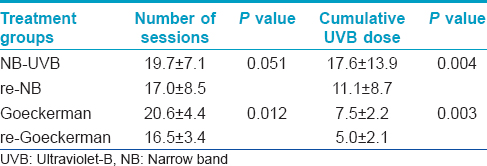
The mean number of phototherapy sessions [Table - 3] was lower in the re-NB-UVB group as compared to NB-UVB the group, but the difference was not statistically significant (P = 0.051). The mean number of sessions in the re-Goeckerman group was significantly lower than Goeckerman group (P = 0.012). The mean cumulative UVB doses [Table - 3] were significantly lower in the retinoid groups compared to NB-UVB and Goeckerman groups respectively without retinoid.
Discussion
Our study demonstrates that Goeckerman therapy is more effective than NB-UVB in the treatment of psoriasis as assessed by the PASI-75 response. The response rates of Goeckerman and re-Goeckerman therapy in our patients (88% and 83%) was similar to previous reports.[3],[4] Different from the conventional Goeckerman therapy, alternative use of NB-UVB instead of broadband UVB is described by some institutions.[1],[2] The only study comparing the efficacies of NB-UVB and Goeckerman therapy we could find was performed with this modified regimen.[2] In this half-body comparison study, Bagel reported that, modified Goeckerman therapy yielded a statistically superior clinical response by the end of the fourth week in comparison to NB-UVB alone.
Acitretin is considered to be the drug of choice for combination with NB-UVB to improve efficacy, safety and tolerability of NB-UVB.[5],[6],[7],[8] In our study the PASI-75 responses of 62% and 39% of patients treated with re-NB-UVB combination and NB-UVB alone were not statistically significant, but the mean number of phototherapy sessions and the cumulative UVB doses in the re-NB-UVB group were lower than NB-UVB monotherapy group. Our response rates were similar to those reported by Ozdemir et al.[9] who reported complete clearance (>PASI-75) in 56.6% after 8 weeks of treatment with re-NB-UVB combination and Kampitak and Asawanonda [8] who reported complete clearance rates of 62.5% vs. 55% for re-NB-UVB and NB-UVB monotherapy groups, respectively.
The PASI-75 response rates of Goeckerman therapy were similar with and without acitretin (88% vs. 83%) but acitretin reduced the number of treatments and cumulative UVB doses delivered.
Although PASI-75 response rates of Goeckerman therapy were also higher than re-NB-UVB group, this difference was not statistically significant.
Combining acitretin with NB-UVB or Goeckerman therapy did not yield a superior efficacy according to PASI-75 response rates in our analysis which might have been due to the small sample size. Aside from efficacy, combining acitretin with Goeckerman therapy resulted in a reduction in the number of sessions and total cumulative doses in our study. We were unable to find any previous study evaluating the combination of acitretin with Goeckerman therapy. Similar to Goeckerman therapy, total delivered UVB doses and number of sessions needed for treatment in the re-NB-UVB group were lower than NB-UVB monotherapy. However, in terms of mean number of sessions, the difference in NB-UVB treatment groups was not statistically significant.
Our study has some limitations. Since this is a retrospective study, the patients were not randomly enrolled and treatment groups have different number of patients and some treatment groups have a relatively low number of patients which makes comparisons difficult.
Conclusion
Goeckerman therapy and NB-UVB phototherapy are very effective phototherapeutic modalities for moderate to severe psoriasis. Our findings suggest that Goeckerman therapy is superior to NB-UVB phototherapy in terms of efficacy. Acitretin enhances the efficacy of both modalities and can reduce the time needed to control disease as well as the total cumulative UV dose.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| 1. |
Gupta R, Debbaneh M, Butler D, Huynh M, Levin E, Leon A, et al. The Goeckerman regimen for the treatment of moderate to severe psoriasis. J Vis Exp 2013;(77):e50509. Doi: 10.3791/50509.
[Google Scholar]
|
| 2. |
Bagel J. LCD plus NB-UVB reduces time to improvement of psoriasis vs. NB-UVB alone. J Drugs Dermatol 2009;8:351-7.
[Google Scholar]
|
| 3. |
Lee E, Koo J. Modern modified 'ultra' Goeckerman therapy: a PASI assessment of a very effective therapy for psoriasis resistant to both prebiologic and biologic therapies. J Dermatolog Treat 2005;16:102-7.
[Google Scholar]
|
| 4. |
Serrao R, Davis MD. Goeckerman treatment for remission of psoriasis refractory to biologic therapy. J Am Acad Dermatol 2009;60:348-9.
[Google Scholar]
|
| 5. |
Lapolla W, Yentzer BA, Bagel J, Halvorson CR, Feldman SR. A review of phototherapy protocols for psoriasis treatment. J Am Acad Dermatol 2011;64:936-49.
[Google Scholar]
|
| 6. |
Lebwohl M, Drake L, Menter A, Koo J, Gottlieb AB, Zanolli M, et al. Consensus conference: Acitretin in combination with UVB or PUVA in the treatment of psoriasis. J Am Acad Dermatol 2001;45:544-53.
[Google Scholar]
|
| 7. |
Carretero G, Ribera M, Belinchón I, Carrascosa JM, Puig L, Ferrandiz C, et al. Guidelines for the use of acitretin in psoriasis. Psoriasis Group of the Spanish Academy of Dermatology and Venereology. Actas Dermosifiliogr 2013;104:598-616.
[Google Scholar]
|
| 8. |
Kampitak T, Asawanonda P. The efficacy of combination treatment with narrowband UVB (TL-01) and acitretin vs narrowband UVB alone in plaque-type psoriasis: a retrospective study. J Med Assoc Thai 2006;89:S20-4.
[Google Scholar]
|
| 9. |
Ozdemir M, Engin B, Baysal I, Mevlitoglu I. A randomized comparison of acitretin-narrow-band TL-01 phototherapy and acitretin-psoralen plus ultraviolet A for psoriasis. Acta Derm Venereol 2008;88:589-93.
[Google Scholar]
|
Fulltext Views
2,385
PDF downloads
848





![[Table - 1]](#tbl_ijdvl_2015_81_6_584_168329_t1.jpg){kind=link}
![[Table - 2]](#tbl_ijdvl_2015_81_6_584_168329_t2.jpg){kind=link}
![[Table - 3]](#tbl_ijdvl_2015_81_6_584_168329_t3.jpg){kind=link}