Translate this page into:
Sunscreens
Correspondence Address:
Anil Abraham
Department of Dermatology, St. John's Medical College Hospital, Bangalore - 560 034
India
| How to cite this article: Kaimal S, Abraham A. Sunscreens. Indian J Dermatol Venereol Leprol 2011;77:238-243 |
Introduction
Sunscreens are a constantly evolving component of the dermatologist′s therapeutic armamentarium. This article attempts to compile some of the important aspects of sunscreens, including their classification, various indices related to photoprotection, and some of the debatable issues related to sunscreens in general. The focus is on material which is current, while at the same time being relevant for the postgraduate.
Indications for the use of Sunscreens
The primary use of sunscreens is to protect the skin from the short-term and long-term effects of ultraviolet radiation. In today′s scenario of procedure-centered dermatology, sunscreens have become an indispensable part of every patient′s post-procedure skin care routine. The characteristics of an ideal sunscreen are listed in [Table - 1]. The common indications for the use of sunscreens in dermatology are in the prevention and management of: [1]
- Sunburn
- Freckling, discoloration
- Photoaging
- Skin cancer
- Phototoxic/ photoallergic reactions
- Photosensitivity diseases
- Polymorphous light eruption (290-365 nm)
- Solar urticaria (290-515 nm)
- Chronic actinic dermatitis (290 nm-visible)
- Persistent light reaction (290-400 nm)
- Lupus erythematosus (290-330 nm)
- Xeroderma pigmentosum (290-340 nm)
- Albinism
- Photoaggravated dermatoses
- Post-inflammatory hyperpigmentation (post-procedure)
Spectrum of UV radiation
The biologically active components of ultraviolet (UV) radiation include UVA and UVB radiation. The primary targets of UV radiation in the skin and their corresponding effects are given below: [2]
UVB (290-320 nm)
- Responsible for the most severe damage
- Direct impact on cell DNA and proteins
- Acute damage - sunburn
- Long-term damage - cancer
UVA (320-400 nm)
- Not directly absorbed by biological targets
- Penetrates deeper than UVB
- Affects connective tissue by producing reactive oxygen species; produces profound immunosuppression
- Responsible for tanning, photoaging, photocarcinogenesis, exogenous photosensitization and many idiopathic photodermatoses (including polymorphous light eruption)
Sea-level solar UV radiation is approximately 95-98% UVA and 2-5% UVB. UVC is completely absorbed by stratospheric ozone that also attenuates UVB. A given solar UVR spectrum varies with the solar zenith angle (the angle between an imaginary perpendicular line and a line from its base to the sun), which is dependent on time of day, season, and latitude. The highest UVB content is found when the sun is directly overhead with the shortest path (e.g., noon, at the equator, at high altitude). [3]
Classification of Sunscreens
The last FDA sunscreen monograph was issued in 1999, with a list of 16 approved sunscreen agents. It recommends that sunscreens be classified as organic and inorganic, replacing the previously used terms "chemical" and "physical", respectively. There are three commonly used nomenclatures for sunscreen agents in the world. These are the International Nomenclature Cosmetic Ingredient (INCI) name, US adopted name (USAN), and trade name. Taking avobenzone (USAN) as an example, the INCI name for avobenzone is butylmethoxydibenzoylmethane, while Parsol 1789 is one of its many trade names. [1],[3],[4],[5]
A. Organic Sunscreens
Organic UV filters are active ingredients that absorb UV radiation within a particular range of wavelengths, depending on their chemical structure. Once the UV filter absorbs energy, it moves from a low-energy ground state to a high-energy excited state. From this excited state, any of the following three processes may occur, depending on the ability of the filter to process the energy it has absorbed:
- Photostable filter: This type of filter dissipates its absorbed energy to the environment as heat energy, and returns to the ground state. It is subsequently fully capable of absorbing UV energy again.
- Photounstable filter: The filter undergoes a change in its chemical structure, or is degraded after absorbing UV energy. It is not capable of absorbing UV energy again.
- Photoreactive filter: In its excited state, the filter interacts with surrounding molecules, including other ingredients of the sunscreen, oxygen, and skin proteins and lipids. This leads to the production of reactive species, which may have unwanted biological effects.
Organic sunscreens are further divided into UVB and UVA filters:
1. UVB filters
- PABA derivatives - Padimate O
- Cinnamates - Octinoxate, Cinoxate
- Salicylates - Octisalate, Homosalate, Trolamine salicylate
- Octocrylene
- Ensulizole
2. UVA filters
- Benzophenones (UVB and UVA2 absorbers) - Oxybenzone, Sulisobenzone, Dioxybenzone
- Avobenzone or Parsol 1789 (UVA1 absorber)
- Meradimate (UVA2 absorber)
Note: Although avobenzone is the only sunscreen agent that has its absorption peak in the UVA1 spectrum (357 nm), making it a very effective UVA filter, it has the disadvantage of being photounstable. This is overcome, to some extent, by adding agents that photostabilize avobenzone, to the final sunscreen product. These agents include other UVA filters such as oxybenzone, UVB filters such as enzacamene (not yet FDA approved), salicylates, octocrylene, broad spectrum filters such as bemotrizinol (not yet FDA approved), and inorganic filters such as titanium dioxide and zinc oxide.
3. Newer generation broad spectrum (UVA + UVB) filters - Ecamsule (Mexoryl SX), Silatriazole (Mexoryl XL), Bemotrizinol (Tinosorb S), Bisoctrizole (Tinosorb M)
Ecamsule is primarily a UVA filter, the patent for which is held by L′Orιal (sunscreens containing ecamsule are exclusive to L′Orιal and its brands). Tinosorb M is the first of a new class of UV filters that combine the properties of both UV conventional filters (organic and inorganic) - it scatters, reflects and absorbs UV light. Apart from Ecamsule, these filters are not yet US FDA approved, but are being used in other countries, such as the European Union and Canada.
B.Inorganic Sunscreens
- Zinc oxide
- Titanium dioxide
- Others - iron oxide, red veterinary petrolatum, kaolin, calamine, ichthammol, talc
Inorganic agents function by reflecting, scattering or absorbing UV radiation. Their opaque nature and "whitening effect" are an inherent disadvantage, which may be minimized by the use of micronized or ultrafine particles.
Systemic Photoprotective Agents
In addition, there are several compounds that have a systemic photoprotective effect; these are sometimes referred to as "systemic sunscreens."
β-carotene, antimalarials, ascorbic acid, α-tocopherols (i.e., vitamins A, C, and E), retinol, selenium, green tea polyphenols, PABA, antihistamines, aspirin, indomethacin, corticosteroids.
Sunscreen-Related Indices [2],[3],[4],[6],[7],[8]Practicing dermatologists often encounter patients complaining of worsening pigmentation or recurrent polymorphous light eruption in spite of using sunscreens with "good sun protection factor (SPF)" or "SPF >50". It is important for both dermatologists and the public to be aware that a good SPF value will not protect the skin from the entire UV spectrum. In fact, in 2007, the FDA has proposed that the expansion of SPF be changed to "sunburn protection factor" to indicate that it is only an index of protection against sunburn or UVB-induced erythema, and hence does not necessarily imply UVA or broad spectrum protection.
Various indices have been formulated by in vitro and in vivo methods to assess the efficacy of sunscreens with respect to specific components of the UV spectrum. These are as follows:
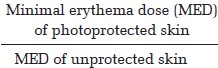
1. UVB sunburn protection factor (SPF) =
Grading system for SPF:
- Low: SPF 2 - 15
- Medium: SPF 15 - 30
- High: SPF 30 - 50
- Highest: SPF >50
Note : It is noteworthy that a sunscreen with an SPF of 15 blocks about 93% of UVB radiation, while one with an SPF of 30 blocks about 97% of UVB radiation. This difference of 4% may make the difference between an aesthetically pleasing sunscreen and an undesirable one, as products with higher SPF generally tend to be uncomfortable due to the higher concentration of the active ingredient. [9]
2. UVA protection indices
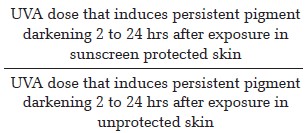
a. Japanese standard (persistent pigment darkening; in vivo method):
b. Australian/New Zealand Standard (in vitro method):
8-μm layer of the product should not transmit more than 10% of radiation of 320 to 360 nm
OR
20-μm layer of the product should not transmit more than 1% of radiation of 320 to 360 nm
c. European Union guidelines:
UVA protection factor (persistent pigment darkening method) = 1/3 of SPF
AND
Critical wavelength = 370 nm
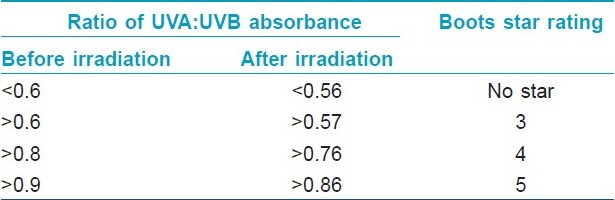
d. Boots star rating system (used in the United Kingdom): In vitro measurement of the ratio of a product′s UVA (320-400 nm) absorbance over its UVB (290-320 nm) absorbance is used to calculate its Boots star rating [Table - 2]. Products with better UVA absorbance have a higher Boots star rating.
3. Immune protection factor (IPF): ability of sunscreen products to prevent UV-induced immunosuppression. IPF is assessed by complex methods such as the ability of a sunscreen to inhibit either the sensitization or elicitation arm of contact or delayed-type hypersensitivity reactions to allergens such as dinitrochlorobenzene (DNCB) and nickel, respectively. IPF is considered to correlate better with the UVA-protectiveness of a sunscreen than with its SPF. [10]
4. Clothing indices
UV protection factor (UPF) = the ratio of average effective UV radiation irradiance transmitted and calculated through air to the average effective UV radiation irradiance transmitted and calculated through fabric (indicates how much longer a person can stay in the sun when fabric covers the skin, erythema being the end-point).
Grading of UPF:
- good protection (UPF 15 to 24)
- very good protection (UPF 25 to 39)
- excellent protection (UPF 40 to 50+)
- Fabric SPF is similar to SPF, except that fabric is used to protect the skin while testing, instead of a sunscreen. [11]
5. Sunglass standards[12]
- Luminous transmittance = Amount of light transmitted through a sunglass lens (e.g. a lens with 20% luminous transmittance allows 20% of the light to pass through it)
- The Australian Standard (AS/NZS 1067:2003) classifies sunglasses and fashion spectacles based on the amount of UV radiation that passes through the lenses:
Categories of lenses: 0 to 4
0 Fashion spectacles (luminous transmittance 80-100%): providing some protection from UV radiation but no reduction in sunglare.
1 Fashion spectacles: providing protection from UV radiation and limited reduction of sunglare - not suitable for driving at night.
2 Sunglasses for general use: providing good protection from UV radiation and sunglare.
3 Sunglasses providing extra protection from UV radiation and sunglare.
4 Sunglasses providing a high level of protection from UV radiation and sunglare (luminous transmittance 3-8%) - must not be used when driving.
- UVB transmittance: 5 percent of luminous transmittance (e.g., for lenses with luminous transmittance of 20 percent, 99 percent of UVB should be blocked out).
- UVA transmittance: lens categories 0 to 2: luminous transmittance, lens categories 3 and 4: 50% of luminous transmittance.
- Minimum vertical diameter for adult sunglasses = 28 mm
- Minimum vertical diameter for child sunglasses = 24 mm
Some sunglasses may also be labeled with an eye protection factor (EPF) number, developed by the Australian Radiation Protection and Nuclear Safety Authority (ARPANSA) ranging from 1 to 10. Sunglasses labeled EPF of 9 or 10 transmit very little UV radiation. Other sunglasses may be labeled UV 400 (blocking 100% of UV) or state the amount of UV radiation blocked as a percentage such as 99.9% or 100%.
The only way to assess the protection of sunglasses is to have the lenses measured, either by the manufacturer or by a properly equipped optician. Dark lenses do not automatically filter out more harmful UV radiation and blue light as compared to light lenses. Inadequate dark lenses are even more harmful than inadequate light lenses (or wearing no sunglasses at all) because they provoke the pupil to open wider. As result, more unfiltered radiation enters the eye. The only "visible" quality test for sunglasses is their fit. For the best protection, one must use wraparound, close fitting, large-lens sunglasses that help to reduce reflected UV radiation and glare that can pass around the edge of the sunglasses and reach the eyes.
Sunscreen-Related Definitions [4],[7],[8]Critical wavelength: The wavelength below which 90% of the sunscreen′s UV absorbency occurs
Broad spectrum sunscreen: Critical wavelength > 370 nm AND UVA protection factor > 4
Water-resistant sunscreen: Maintains the label SPF value after two sequential immersions in water for 20 min (40 min)
Very water-resistant sunscreen: Maintains the label SPF value after four sequential immersions in water for 20 min (80 min)
In the United States, a product that has been shown to be water-resistant or very water-resistant, can also be labeled as "sweat resistant."
Recommendations for Sunscreen Application
Sunscreen should be applied properly to all sun exposed areas (in a concentration of 2 mg/cm 2 ), and allowed to dry completely before sun exposure. It should be reapplied every 2 hours, and after swimming, vigorous activity, excessive perspiration, or toweling.
"Teaspoon rule": [13]
3 mL (slightly more than half a teaspoon)
- for each arm
- for the face and neck
6 mL (slightly more than a teaspoon)
- for each leg
- for the chest
- for the back
Debatable Issues
1. Sunscreen use in infants
Although not known to be hazardous, the use of sunscreens is not recommended for infants younger than 6 months. [3]
2. Contact dermatitis
The most common cause of contact dermatitis (photoallergy) among sunscreens is oxybenzone. [3]
3. Nanosized particles
Nanosized particles range in size from 1-100 nm. Microfine forms of zinc oxide and titanium dioxide have a particle size of 20-50 nm. Nanotechnology makes inorganic sunscreens more cosmetically acceptable (less whitening of skin after application). In recent years, there have been concerns that nanoparticles can induce free radical formation in the presence of UV radiation. However, studies show that these particles remain on the surface of the skin or in the stratum corneum, and are hence safe for human use. [4]
4. Vitamin D production
UVB radiation is responsible for more than 90% of vitamin D production in the skin. It is said that a few minutes exposure of the face, arms, and hands to noonday summer sunlight two or three times a week is sufficient for vitamin D synthesis. [14] There have been concerns that widespread use of sunscreens, particularly those with high SPF, may lead to a significant decrease in vitamin D production. However, there is evidence that though sunscreens can significantly reduce the production of vitamin D under very strictly controlled conditions, their normal usage does not generally result in vitamin D insufficiency. [15] In fact, vitamin D and calcium levels have been found to be relatively normal in xeroderma pigmentosum patients, in spite of strict photoprotection. [16]
5. Hormonal effects
Some sunscreens (oxybenzone, avobenzone, octinoxate, padimate O) have been tested for their estrogenic/anti-androgenic properties in animal studies. [4] However, the endocrine effects of these agents remain controversial, warranting further human studies.
New Sunscreen Technologies [17]
SunSpheres
SunSpheres are styrene/acrylate copolymers that do not absorb UV irradiation but enhance the effectiveness of the active sunscreen ingredients. The SunSphere polymer beads are filled with water, which migrates out of the particle, leaving behind tiny air-filled spheres, which have a lower refractive index (1.0) than the dried sunscreen film (1.4-1.5). As a result, scattering of UV radiation occurs, increasing the probability of contact with the active UV filters in the sunscreen. SunSpheres are also available in a powder form, and can boost SPF by 50 -70% making it possible to reduce the concentration of active ingredients.
Microencapsulation
Active sunscreen ingredients are entrapped within a silica shell, as a result of which, allergic or irritant reactions to the active ingredient can be minimized, and incompatible sunscreen ingredients can be safely combined, without loss of efficacy.
Suggested sources for further reading:
1. Cutaneous photobiology: Fitzpatrick′s dermatology in general medicine (7 th edition) - Chapters 88 and 89.
2. Good reviews on sunscreens:
- Dermatologic Clinics 2006, Issue 1 - all articles
- Rai R, Srinivas CR. Photoprotection. Indian J. Dermatol. Venereol. Leprol. 2007; 73: 73-9.
- Antoniou C, Kosmadaki MG, Stratigos AJ, Katsambas AD. Sunscreens- what′s important to know. J. Eur. Acad. Dermatol. Venereol. 2008; 22: 1110-8.
3. Systemic photoprotection
- Anstey AV. Systemic photoprotection with alpha-tocopherol (vitamin E) and beta-carotene. Clin. Exp. Dermatol. 2002; 27: 170-6.
- Sies H, Stahl W. Carotenoids and UV protection. Photochem Photobiol Sci. 2004; 3: 749-52.
| 1. |
Levy SB. Sunscreens. In: Wolverton SE, editor. Comprehensive dermatologic drug therapy. 2 nd ed. Philadelphia: Saunders; 2007. p. 703-18.
[Google Scholar]
|
| 2. |
Forestier S. Rationale for sunscreen development. J Am Acad Dermatol 2008;58:S133-8.
[Google Scholar]
|
| 3. |
Lim HW. Photoprotection and sun-protective agents. In: Wolff K, Goldsmith LA, Katz SI, Gilchrest BA, Paller AS, Leffell DJ, editors. Fitzpatrick′s dermatology in general medicine. 7 th ed. New York: McGraw-Hill; 2008. p. 2137-41.
[Google Scholar]
|
| 4. |
Hexsel CL, Bangert SD, Hebert AA, Lim HW. Current sunscreen issues: 2007 Food and Drug Administration sunscreen labelling recommendations and combination sunscreen/insect repellent products. J Am Acad Dermatol 2008;59:316-23.
[Google Scholar]
|
| 5. |
Lowe NJ. An overview of ultraviolet radiation, sunscreens, and photo-induced dermatoses. Dermatol Clin 2006;24:9-17.
[Google Scholar]
|
| 6. |
Wang SQ, Stanfield JW, Osterwalder U. In vitro assessments of UVA protection by popular sunscreens available in the United States. J Am Acad Dermatol 2008;59:934-42.
[Google Scholar]
|
| 7. |
Lim HW, Naylor M, Hönigsmann H, Gilchrest BA, Cooper K, Morison W, et al. American academy of dermatology consensus conference on UVA protection of sunscreens: Summary and recommendations. J Am Acad Dermatol 2001;44:505-8.
[Google Scholar]
|
| 8. |
Rai R, Srinivas CR. Photoprotection. Indian J Dermatol Venereol Leprol 2007;73:73-9.
[Google Scholar]
|
| 9. |
Draelos ZD. Compliance and sunscreens. Dermatol Clin 2006;24:101-4.
[Google Scholar]
|
| 10. |
Fourtanier A, Moyal D, Maccario J, Compan D, Wolf P, Quehenberger F, et al. Measurement of sunscreen immune protection factors in humans: A consensus paper. J Invest Dermatol 2005;125:403-9.
[Google Scholar]
|
| 11. |
Hatch KL, Osterwalder U. Garments as solar ultraviolet radiation screening materials. Dermatol Clin 2006;24:85-100.
[Google Scholar]
|
| 12. |
Standards Australia [homepage on the Internet]. Sydney: Standards Australia Limited; c2010. Available from: http://www.standards.org.au/ [Last cited on 2010 Jun 18].
[Google Scholar]
|
| 13. |
Schneider J. The teaspoon rule of applying sunscreen. Arch Dermatol 2002;138:838-9.
[Google Scholar]
|
| 14. |
Young AR, Walker SL. Acute and chronic effects of ultraviolet radiation on the skin. In: Wolff K, Goldsmith LA, Katz SI, Gilchrest BA, Paller AS, Leffell DJ, editors. Fitzpatrick′s dermatology in general medicine. 7 th ed. New York: McGraw-Hill; 2008. p. 2137-41.
[Google Scholar]
|
| 15. |
Norval M, Wulf HC. Does chronic sunscreen use reduce vitamin D production to insufficient levels? Br J Dermatol 2009;161:732-6.
[Google Scholar]
|
| 16. |
Sollitto RB, Kraemer KH, DiGiovanna JJ. Normal vitamin D levels can be maintained despite rigorous photoprotection: Six years′ experience with xeroderma pigmentosum. J Am Acad Dermatol 1997;37:942-7.
[Google Scholar]
|
| 17. |
Antoniou C, Kosmadaki MG, Stratigos AJ, Katsambas AD. Sunscreens- what′s important to know. J Eur Acad Dermatol Venereol 2008;22:1110-8.
[Google Scholar]
|
Fulltext Views
31,262
PDF downloads
8,714





![[Table - 1]](#tbl_ijdvl_2011_77_2_238_77480_t1.jpg){kind=link}
![[Table - 2]](#tbl_ijdvl_2011_77_2_238_77480_t2.jpg){kind=link}