Translate this page into:
Primary tuberculosis of glans penis after intravesical Bacillus Calmette Guerin immunotherapy
2 Department of Urology, All India Institute of Medical Sciences, New Delhi, India
3 Department of Microbiology, All India Institute of Medical Sciences, New Delhi, India
4 Department of Pathology, All India Institute of Medical Sciences, New Delhi, India
Correspondence Address:
V K Sharma
Department of Dermatology and Venereology, All India Institute of Medical Sciences, New Delhi - 110 029
India
| How to cite this article: Sharma V K, Sethy P K, Dogra P N, Singh U, Das P. Primary tuberculosis of glans penis after intravesical Bacillus Calmette Guerin immunotherapy. Indian J Dermatol Venereol Leprol 2011;77:47-50 |
Abstract
A 55-year-old male with carcinoma in situ of urinary bladder was treated with weekly intravesical injections of Bacillus Calmette Guerin (BCG) vaccine. Three days after the sixth injection, he developed low grade fever and multiple grouped punched out, 2-3 mm ulcers around meatus and corona glandis. In addition, multiple, firm, indurated, nontender papules and few deeper nodules were present on the proximal part of glans penis, along with bilateral enlarged, matted and nontender inguinal lymph nodes. There was no history suggestive of sexually transmitted diseases and high risk behavior. Chest X-ray was within normal limits, and Mantoux, Venereal Disease Research Laboratory (VDRL) and HIV antibody tests were negative. The biopsy from the penile ulcer revealed epithelioid cell granuloma with Langhans giant cells. Fine needle aspiration cytology from the lymph node also revealed epithelioid cell granuloma and acid fast bacilli on Ziehl Neelsen's stain. The tissue biopsy grew Mycobacterium tuberculosis. The BCG immunotherapy was stopped and patient was treated with four drug antitubercular therapy with isoniazid, rifampicin, ethambutol, and pyrazinamide in standard daily doses along with pyridoxine. The edema resolved and the ulcers started healing within 2 weeks, and at 6 weeks after starting antitubercular therapy almost complete healing occurred. To the best of our knowledge, we describe the first case of an Indian patient with BCG induced primary tuberculosis of penis after immunotherapy for carcinoma urinary bladder and review the previously described cases to increase awareness of this condition in dermatologists and venereologists.Introduction
Bacillus Calmette Guerin (BCG) is a live attenuated strain of Mycobacterium bovis, and is used for the treatment of superficial and in situ carcinoma of urinary bladder, residual bladder tumor left after surgical resection and prophylaxis of multiple and/or recurrent bladder tumors. [1] Primary infection of glans penis is an extremely rare complication of this therapy and we report here one such case. [2],[3],[4],[5],[6],[7],[8],[9],[10],[11],[12],[13]
Case Report
A 55-year-old man who was diagnosed with carcinoma in situ of urinary bladder and treated with weekly intravesical injections of BCG vaccine (80 mg) was referred to our venereology clinic for redness, pain and ulceration of glans penis. Symptoms were noted 3 days after the sixth sitting of BCG instillation. This last sitting of intravesical therapy was associated with difficulty in insertion of the catheter and traumatic bleeding. There was no past history of tuberculosis. On examination, he had multiple grouped punched out ulcers of size 2-3 mm in the peri-meatal location. Similar discrete ulcers were present on corona glandis [Figure - 1] and [Figure - 2]. Multiple, firm, indurated, nontender papules and few deeper nodules on the proximal part of glans penis were also present. The whole of penis including the glans was edematous. Bilateral inguinal lymph nodes were enlarged, with size varying from 3 to 5 cm, matted and nontender. There was no fluctuation. No other lymph nodes in the body were enlarged. There was no history of premarital or extramarital sexual exposure. There was no history of genital ulceration in the past. He had low grade fever and malaise at the time of presentation but there was no history of weight loss or chronic cough. Chest X-ray was within normal limits, and Mantoux was 8 mm at 48 hours. Tzanck smear for multinucleated giant cells as well as Venereal Disease Research Laboratory (VDRL) and HIV antibody tests were negative. Culture for herpes simplex virus was not done.
 |
| Figure 1 :Bacillus Calmette Guerin induced balanitis: Multiple ulcers of size 2– 3 mm in the peri-meatal location |
 |
| Figure 2 :Bacillus Calmette Guerin induced balanitis: Multiple ulcers spreading from meatus along the posterior surface of glans penis to corona glandis |
The biopsy from the penile ulcer revealed epithelioid cell granuloma with Langhans giant cells [Figure - 3]a and b. Fine needle aspiration cytology (FNAC) from the lymph node also revealed epithelioid cell granuloma [Figure - 3]c and acid fast bacilli (AFB) on Ziehl Neelsen′s stain [Figure - 3]d. The tissue biopsy subjected for mycobacterial culture had grown Mycobacterium tuberculosis; however, the polymerase chain reaction (PCR) for M. tuberculosis and M. bovis was negative.
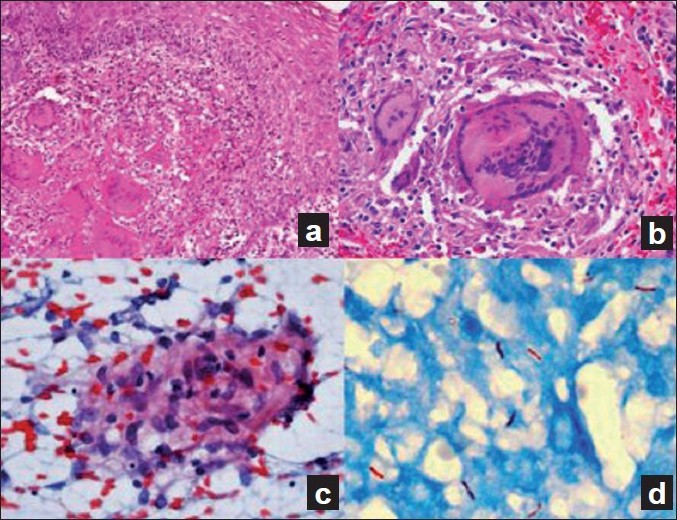 |
| Figure 3 :(a) Section showing epithelioid cell granuloma with Langhans giant cells (H and E, ×200); (b) Section showing epithelioid cell granuloma with Langhans giant cells (H and E, ×400); (c) FNAC from inguinal lymph nodes showing epitheloid cell granuloma (Giemsa, ×40); (d) FNAC from inguinal lymph nodes showing AFB (Ziehl Neelsen, ×1000) |
The BCG immunotherapy was withheld and we initiated therapy with isoniazid 300 mg/day, rifampicin 450 mg/day, ethambutol 800 mg/day, pyrazinamide 1500 mg/day, and pyridoxine 20 mg/day. The edema resolved and the ulcers healed when the patient was evaluated 2 weeks after starting antitubercular therapy. There was almost complete re-epithelization after 6 weeks of antitubercular therapy [Figure - 4].
 |
| Figure 4 :Healing Bacillus Calmette Guerin induced balanitis: Post antitubercular treatment at 6 weeks |
Discussion
BCG is a live, attenuated organism used to provide protective immunity against tuberculosis. It is administered intradermally in children, and it limits the primary infection to subclinical proportions and also appears to protect against disseminated tuberculosis. It is also used to confer immunity against Mycobacterium leprae, either alone or in combination with killed M. leprae. Intravesical instillation of BCG is a widely accepted immunotherapeutic modality of superficial and in situ transitional cell carcinoma of urinary bladder. BCG immunotherapy has also been described for the treatment of malignant melanoma. Since it is a live attenuated vaccine; it should not be administered to patients with immunocompromised status.
A large number of local and generalized reactions have been reported after BCG vaccination. Nonspecific reactions include urticaria, erythema multiforme, generalized maculopapular or purpuric eruption, extensive and protracted ulceration. Specific reactions include lupus vulgaris, lichen scrofulosorum, papulonecrotic tuberculid, development of basal cell carcinomas and disseminated cutaneous granulomas. [12] Distant cutaneous granulomas have been reported after BCG immunotherapy for malignant melanoma. [11]
BCG intravesical therapy may cause minor reactions like cystitis, hematuria, low-grade fever, malaise and nausea. Major side effects include fever >39.5C, granulomatous pneumonitis, hepatitis, bladder contracture, renal abscess and fatal sepsis. [12]
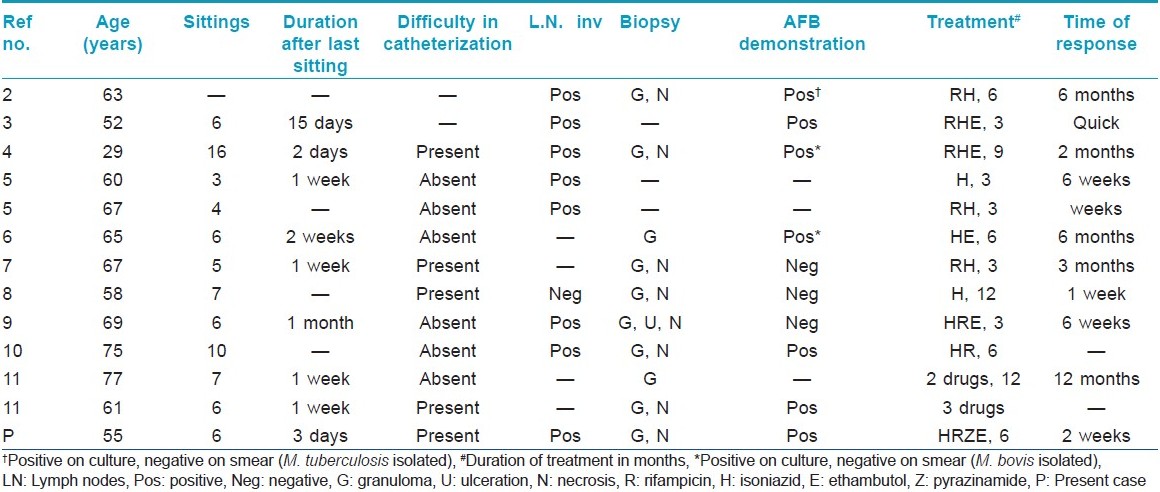
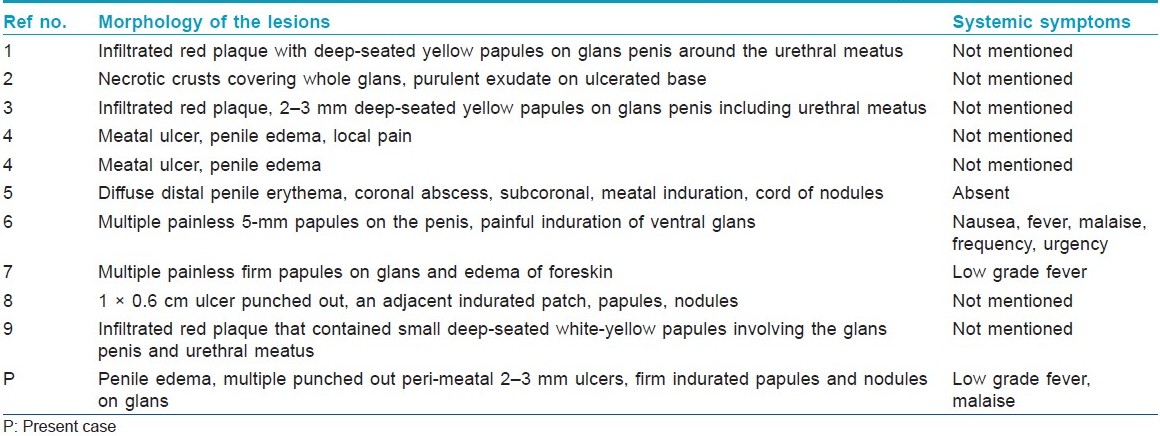
Occurrence of balanitis and penile ulcers is a rare complication of intravesical instillation of BCG. It was first described by Kohona et al. in 1992 in a 63-year-old man. However, the culture of the tissue grew M. tuberculosis. So, they concluded that their case represents primary tuberculosis of glans penis. [2] Thereafter, it has been described in 11 more patients so far. The clinical features of these patients are summarized in [Table - 1] and [Table - 2]. The patients developed these complaints after 3-16 sittings of BCG intravesical instillation. Most of the patients had associated inguinal lymphadenopathy, and biopsy from the ulcer revealed granulomatous inflammation. It should be noted that in addition to multiple ulcers on the glans, most of the patients had indurated plaques, deep-seated papules, nodules, nodules coalescing to form cords rendering a granulomatous clinical appearance to the genital lesions. French et al. have concluded that their patient had papulonecrotic tuberculids induced by BCG, whereas other workers have described their cases as granulomatous balanitis or balanoposthitis or meatal ulceration.
The draining inguinal lymph nodes were usually enlarged bilaterally or unilaterally. In our case, they were matted together. The occurrence of these lesions within days to weeks after the therapy provides evidence that BCG M. bovis is the pathogenetic agent. It seems that traumatic catheterization predisposes to the development of primary infection and consequently balanitis.
Of all these cases, one case demonstrated the growth of M. tuberculosis, [2] while two cases demonstrated the growth of BCG M. bovis on tissue culture. [4],[6] In our patient, the tissue culture grew M. tuberculosis, so we conclude that he had primary tuberculosis of glans penis after intravesical instillation of BCG, as described before by Yoshida et al. [10] The plausible explanation for this could be that either traumatic BCG inoculation predisposes to tubercular infection or BCG undergoes some mutational changes to acquire M. tuberculosis like characteristics. The PCR for M. tuberculosis was negative and it was found to be of low specificity and sensitivity in cutaneous tuberculosis in another study carried out at our institute. [14] It also emphasizes the fact that BCG-induced granulomatous balanoposthitis should be given four drug regimen to prevent systemic dissemination.
To the best of our knowledge, we describe the first Indian patient with this entity and re-emphasize that the dermatologists and venereologists be aware of this entity for accurate diagnosis and adequate treatment as BCG immunotherapy is a widely used and efficacious treatment modality for superficial and in situ carcinoma of urinary bladder.
The risk of BCG balanitis or very rarely primary tuberculosis of glans does not warrant the withdrawal of modality in carcinoma urinary bladder, but the BCG immunotherapy has to be stopped and antitubercular therapy initiated as soon as possible. Careful and atraumatic intravesical BCG instillation can reduce the risk of its complications.
| 1. |
Jones JS, Campbell SC. Non-muscle-invasive bladder cancer (Ta, T1 and CIS). In: Wein AJ, Kavoussi LR, Novick AC, Partin AW, Peters CA, editors. Campbell-Walsh Urology. 9 th ed. Philadelphia: Saunders Elsevier; 2007. p. 2447-67.
[Google Scholar]
|
| 2. |
Konohana A, Noda J, Shoji K, Hanyaku H. Primary tuberculosis of the glans penis. J Am Acad Dermatol 1992;26:1002-3.
[Google Scholar]
|
| 3. |
Erol A, Ozgur S, Tahtali N, Akbay E, Dalva I, Cetin S. Bacillus Calmette-Guerin (BCG) balanitis as a complication of intravesical BCG immunotherapy: A case report. Int Urol Nephrol 1995;27:307-10.
[Google Scholar]
|
| 4. |
Ribera M, Bielsa J, Manterola JM, Fernandez MT, Ferrandiz C. Mycobacterium bovis-BCG infection of the glans penis: A complication of intravesical administration of bacillus Calmette-Guerin. Br J Dermatol 1995;132:309-10.
[Google Scholar]
|
| 5. |
Baniel J, Lev Z, Engelstein D, Servadio C. Penile edema and meatal ulceration after intravesical instillation with bacillus Calmette-Guerin. Urology 1996;47:932-4.
[Google Scholar]
|
| 6. |
Latini JM, Wang DS, Forgacs P, Bihrle W 3 rd . Tuberculosis of the penis after intravesical bacillus Calmette-Guerin treatment. J Urol 2000;163:1870.
[Google Scholar]
|
| 7. |
French CG, Hickey L, Bell DG. Caseating granulomas on the glans penis as a complication of bacillus Calmette Guerin intravesical therapy. Rev Urol 2001;3:36-8.
[Google Scholar]
|
| 8. |
Hattori Y, Hara Y, Matsuura K, Hasegawa A. Granulomatous balanoposthitis after intravesical bacillus Calmette Guerin instillation therapy. Int J Urol 2006;13:1361-3.
[Google Scholar]
|
| 9. |
Kureshi F, Kalaaji AN, Halvorson L, Pittelkow MR, Davis MD. Cutaneous complications of intravesical treatments for bladder cancer: Granulomatous inflammation of the penis following BCG therapy and penile gangrene following mitomycin therapy. J Am Acad Dermatol 2006;55:328-31.
[Google Scholar]
|
| 10. |
Yoshida R, Kawasaki H, Miyajima A, Amagai M, Ohyama M. Primary tuberculosis of the penis after intravesical bacillus Calmette-Guerin instillation therapy. J Eur Acad Dermatol Venereol 2009;23:77-8.
[Google Scholar]
|
| 11. |
Yates VM, Rook GA. Mycobacterial infections. In: Champion RH, Burton JL, Burns DA, Breathnach SM, editors. Textbook of Dermatology. 7 th ed. Oxford: Blackwell Science; 2004. p. 28.7.
[Google Scholar]
|
| 12. |
Lamm DL, van der Meijden PM, Morales A, Brosman SA, Catalona WJ, Herr HW, et al. Incidence and treatment of complications of bacillus Calmette-Guerin intravesical therapy in superficial bladder cancer. J Urol 1992;147:596-600.
[Google Scholar]
|
| 13. |
Michelet N, Spenatto N, Viraben R, Cuny JF, Mazet J, Trechot P, et al. BCG infection of glans penis after intravesical BCG therapy. Ann Dermatol Venereol 2008;135:479-83.
[Google Scholar]
|
| 14. |
Suthar C. Evaluation of mRNA PCR as diagnostic modality for cutaneous tuberculosis. New Delhi: Thesis submitted at All India Institute of Medical Sciences; 2008.
[Google Scholar]
|
Fulltext Views
4,085
PDF downloads
1,184





![[Figure - 1]](#fig_ijdvl_2011_77_1_47_74979_f3.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2011_77_1_47_74979_f4.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2011_77_1_47_74979_f5.jpg){kind=link}
![[Figure - 4]](#fig_ijdvl_2011_77_1_47_74979_f6.jpg){kind=link}
![[Table - 1]](#tbl_ijdvl_2011_77_1_47_74979_t1.jpg){kind=link}
![[Table - 2]](#tbl_ijdvl_2011_77_1_47_74979_t2.jpg){kind=link}