Translate this page into:
Clinical and pathological characterization of oral mucosal 'lichen planus-like lesions' in patients with pemphigus vulgaris: An observational study
2 Department of Histopathology, Postgraduate Institute of Medical Education and Research, Chandigarh, India
3 Department of Biostatistics, Postgraduate Institute of Medical Education and Research, Chandigarh, India
Correspondence Address:
Dipankar De
Department of Dermatology, Venereology and Leprology, Postgraduate Institute of Medical Education and Research, Chandigarh - 160 012
India
| How to cite this article: De D, Arora AK, Handa S, Chatterjee D, Saikia UN, Radotra BD, Kishore K, Khullar G. Clinical and pathological characterization of oral mucosal 'lichen planus-like lesions' in patients with pemphigus vulgaris: An observational study. Indian J Dermatol Venereol Leprol 2020;86:278-283 |
Abstract
Background: Lichen planus-like lesions on oral mucosa occasionally occur in Indian patients with pemphigus vulgaris. Its significance, both clinical and pathological, is yet to be elucidated.
Aims and Objectives: To study the clinical and pathological characteristics of clinically apparent oral mucosal lichen planus-like lesions in pemphigus patients and to assess their relation with pemphigus disease activity.
Materials and Methods: A total of 32 patients with pemphigus vulgaris who had oral lichen planus-like lesions were included and classified as 'cases,' and eight diagnosed cases of pemphigus vulgaris without lichenoid 'hue' were included as controls. The biopsy specimens were subjected to routine histopathologic examination, immunohistochemistry with FasL, and caspase-3 and direct immunofluorescence.
Results: On histopathologic examination, the diagnosis of pemphigus vulgaris, lichen planus, 'overlap' and 'nonspecific' were rendered in 19 (59.4%), 4 (12.5%), 5 (15.6%) and 4 (12.5%) cases, respectively. On immunohistochemistry, FasL was positive in epithelial cells in 16 (50%) cases and 4 (12.5%) controls (P = 0.066). Caspase-3 stained positively in 18 (56.2%) cases and 20 (62.5%) controls (P = 0.77). Direct immunofluorescence was positive in 77.8% (21/27) of the cases.
Limitations: Relatively small number of controls is the limitation of this study.
Conclusion: Lichen planus-like lesions in pemphigus should not be labeled as inactive disease or postinflammatory hyperpigmentation. Apoptosis followed by pigment incontinence seems to explain such lesions with 'lichen planus-like appearance' in oral pemphigus vulgaris. Active pemphigus smoulders in a majority of these lesions.
Introduction
Postinflammatory hyperpigmentation of the skin is common in Indian patients with pemphigus. Similar to postinflammatory hyperpigmentation of any other etiology, it is brownish in color and generally limited to the sites of healed erosions of pemphigus. Occasionally, lichen planus-like lesions occur on oral mucosa in Indian patients with pemphigus vulgaris. Until now, these have been ignored as postinflammatory hyperpigmentation. Moreover, if a prior diagnosis of pemphigus vulgaris is not known, often these are erroneously labeled as oral lichen planus. These pigmentary abnormalities have not been studied systematically earlier.
Apoptosis of epidermal keratinocytes has been proposed as one of the basic mechanisms of acantholysis in experimental models of pemphigus pathogenesis. Apoptosis of keratinocytes is commonly observed in lichen planus histopathology. Apoptosis may thus be a common link between pemphigus vulgaris and lichen planus. The objectives of the study were to clinically and histologically characterize the lichen planus-like lesions on oral mucosa in pemphigus vulgaris patients, to determine whether such pigmentation represents inactive postinflammatory hyperpigmentation or active disease of pemphigus and finally to assess the status of apoptosis by using immunohistochemistry markers of apoptosis in human mucosal biopsy specimens.
Materials and Methods
The approval for the study was obtained from the Institute Ethics Committee (extramural) of the Postgraduate Institute of Medical Education and Research, Chandigarh, India before initiation of the study. Previously diagnosed cases of pemphigus vulgaris (Tzanck smear positive with characteristic histopathology findings and intercellular deposits on direct immunofluorescence) registered to the Immunobullous Disease Clinic of the Department of Dermatology of Postgraduate Institute of Medical Education and Research, Chandigarh were checked for eligibility for inclusion in the study. The inclusion criteria were diagnosed cases of pemphigus vulgaris with violaceous hue, violaceous streaks, reticulate pattern or violaceous plaques anywhere in oral mucosa, irrespective of disease activity elsewhere or ongoing treatment. Patients with dental amalgam in situ, history of smoking or tobacco/betel leaf or areca nut chewing, sharp tooth impinging on the lichen planus-like lesion, current intake of drugs (excluding those for pemphigus) known to cause oral mucosal pigmentary changes were excluded from the study. Diagnosed cases of pemphigus vulgaris without lichenoid 'hue' were included as controls. After obtaining informed consent from eligible patients, a 2.5 mm punch biopsy was obtained from one of the lichen planus-like lesions for histopathologic examination and immunohistochemistry with FasL and caspase-3. Another 2.5 mm punch biopsy was taken from the normal looking mucosa adjoining the mucosal lichen planus-like lesion, from where biopsy for histopathological examination was taken, to perform direct immunofluorescence in order to check for the presence of immunological activity of pemphigus vulgaris. For controls, biopsy for histopathological examination was taken from the margin of an active erosion and for direct immunofluorescence it was taken from normal looking mucosa.
Hematoxylin and eosin and immunohistochemistry slides [(anticaspase-3 antibody clone E 87, ab 32351), (anti-Fas ligand antibody, ab 68338)] were prepared following the routine procedure.
The histopathology and immunohistochemistry slides were interpreted by two pathologists. The diagnosis rendered on histopathology and score assigned on immunohistochemistry were based on consensus between them. A histopathological diagnosis of pemphigus vulgaris was rendered when there was suprabasal bulla or acantholytic cells or tombstoning or a combination of the above. A diagnosis of lichen planus was rendered when there was basal cell vacuolization and/or band-like lymphomononuclear infiltrate in the superficial subepithelium. A diagnosis of 'overlap' (pemphigus vulgaris/lichen planus) or 'nonspecific' was assigned when features of both the entities or none were present, respectively.
Results
A total of 32 cases [Figure - 1]a, [Figure - 1]b, [Figure - 1]c, [Figure - 1]d and eight controls were recruited for the study. Among the 32 cases, eight were males and 24 were females (M/F = 1:3). Of the eight controls, two were males and six were females (M/F = 1:3). The gender distribution was not significantly different. The mean age of cases was 50.39 ± 10.36 years, whereas that of the controls was 33.75 ± 15 years. Thus, the cases were significantly older than the controls (P = 0.001; t-test).
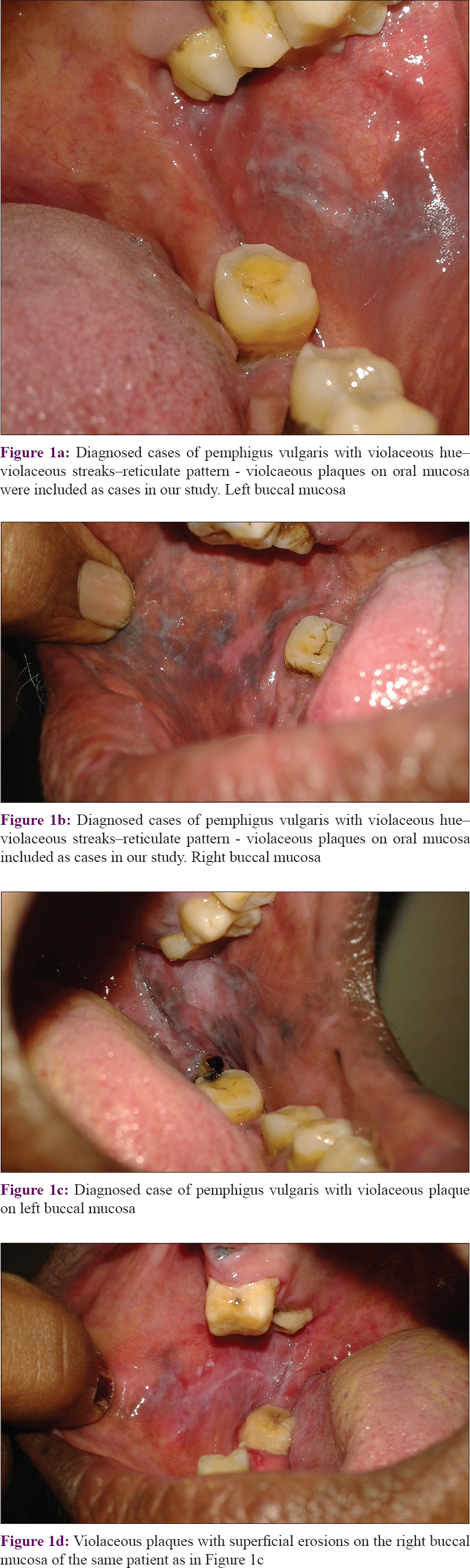 |
| Figure 1: |
The average duration of mucosal pemphigus in cases was 41.61 ± 39.66 months, whereas in controls it was much shorter at 18 ± 16.9 months and the difference was statistically significant (P = 0.017; t-test). There was no significant difference in the proportion of patients receiving cyclophosphamide (which can cause mucosal pigmentation) between the cases and controls (8, 25% vs 1, 12.5%, P = 0.41; Fisher's exact test). Direct immunofluorescence could be interpreted in 27 cases, out of which 21 (77.8%) showed positive results. In the remaining five cases, biopsy tissue was scanty for conclusive reporting of direct immunofluorescence.
The details of histopathological examination and direct immunofluorescence are presented in [Table - 1]. On histopathological examination [Figure - 2], [Figure - 3], [Figure - 4], the diagnosis of pemphigus vulgaris, lichen planus, 'overlap' and 'nonspecific' were rendered in 19 (59.4%), 4 (12.5%), 5 (15.6%) and 4 (12.5%) cases, respectively, whereas the corresponding figures in the control group were 4 (50%), 0 (0%), 3 (37.5%) and 1 (12.5%), respectively. Altogether, histopathological features of pemphigus vulgaris were present in 75% of the cases and 87.5% of the controls.

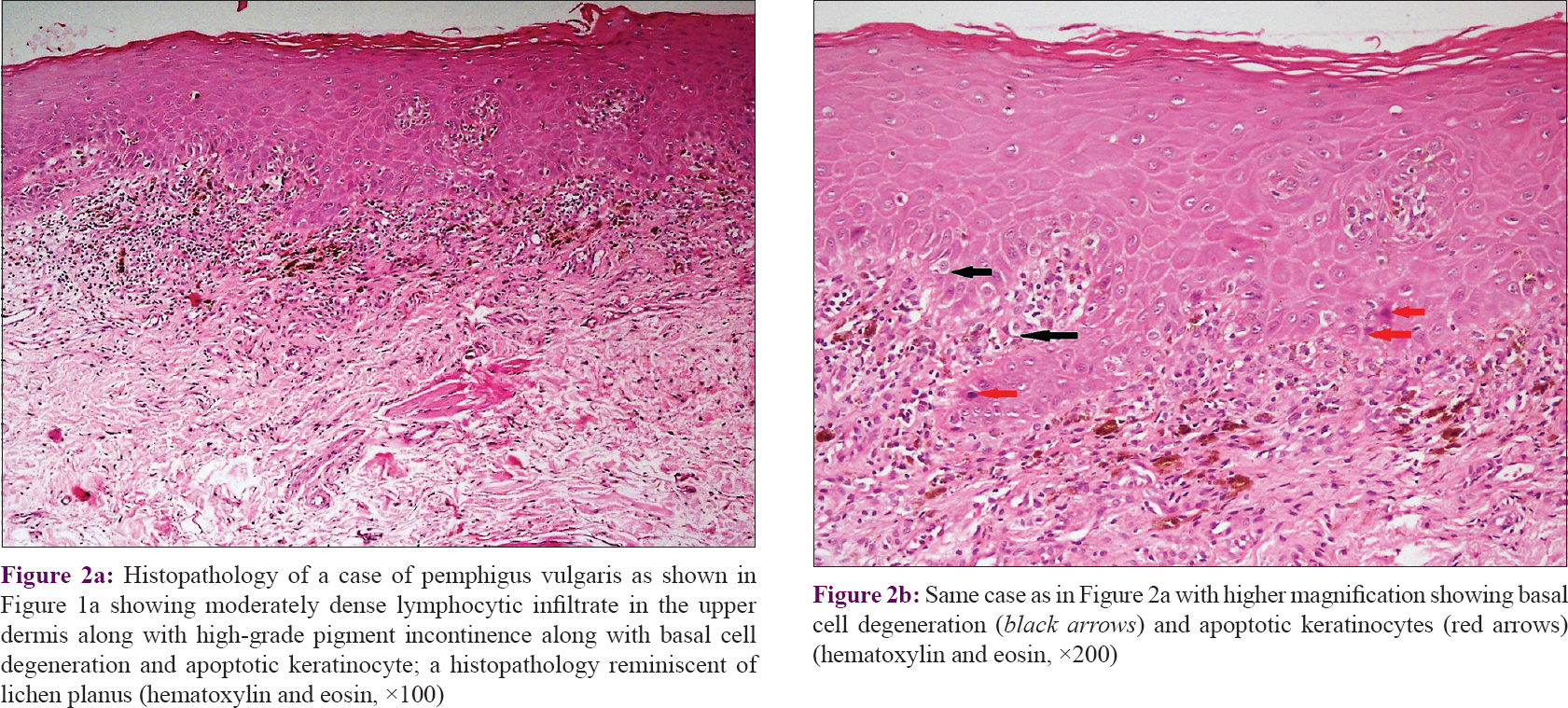 |
| Figure 2: |
 |
| Figure 3: |
 |
| Figure 4: |
On immunohistochemistry, FasL was positive in 50% (16) of the cases and 12.5% (1) of the controls (P = 0.066; Fisher's exact test). Although the FasL positivity was numerically more common in patients with lichen planus-like lesions, the difference did not attain statistical significance. Caspase-3 stained positively in 18 (56.2%) cases and 5 (62.5%) controls (P = 0.78). However, a higher degree of positivity (3+) was seen only in cases and none in controls.
Discussion
Clinically apparent lichen planus-like lesions are occasionally seen on the oral mucosa of patients with pemphigus vulgaris. It is usually trivialized as inactive disease or postinflammatory hyperpigmentation and equated with postinflammatory hyperpigmentation observed on the skin of patients with pemphigus vulgaris. This study provides some interesting initial insights into this previously undescribed uncommon clinical observation.
From the demographic point of view, it was seen that cases with lichen planus-like lesions were significantly older and had a disease duration significantly longer than the pemphigus vulgaris patients who did not have lichen planus-like lesions. There are two possible hypotheses for this observation: (a) chronic inflammation leads to pigmentation as can be seen with any other inflammatory dermatoses on the skin of color,[1] (b) lichen planus-like lesions simply represent chronicity of the disease.[2] In a recently published study, we have observed that lichen planus-like lesions of oral pemphigus vulgaris are associated with treatment refractoriness.[2] Ignoring these lesions as inactive postinflammatory hyperpigmentation may lead to premature tapering of treatment, which may result in early aggravation of active disease. On histopathological observation of the features of pemphigus vulgaris in 75% of the cases and that on direct immunofluorescence in 77.8% of the evaluable specimen, it is suggested that they represent active disease and treatment decisions should be made after atleast a histopathological examination of a biopsy specimen is done.
Apoptosis has been claimed to be the initiator of acantholysis in pemphigus in variousin vitro studies.[3],[4],[5],[6],[7],[8],[9],[10],[11],[12],[13] However, supporting data fromin vivo studies is lacking.[12],[13] To determine the prevalence and significance of apoptosis, we carried out immunohistochemistry studies with two important markers of apoptosis, namely FasL and caspase-3. A total of 17 out of 40 (42.5%) patients with pemphigus (cases and controls) showed positive staining pattern for FasL. Similarly, 23 out of 40 (57.5%) patients with pemphigus showed positive staining for caspase-3. Thus, a high prevalence of apoptosis marker positivity was seen in patients with pemphigus which suggests that it is an important mechanism of acantholysis in pemphigus, as claimed in earlierin vitro studies.
The pigmentation is perhaps the result of apoptosis of basal cells/other keratinocytes and melanin incontinence irrespective of lichenoid infiltrate. Apoptotic keratinocytes were observed in nearly 10% of the cases even on routine histopathology. Although lymphocytic infiltrate was seen in 53.12% of the cases, it was observed in 87.5% of the controls as well. A band-like lichenoid infiltrate was present in 18.75% cases vs 37.5% positive controls. Inflammation does occur in the superficial subepithelium in pemphigus but that cannot explain the lichen planus-like pigmentation as such. Hypothetically, antigen unmasking by acantholysis and apoptosis of epithelial keratinocytes may lead to lichenoid inflammation which may explain lichen planus/pemphigus vulgaris overlap on histopathology. In addition to the inflammation, pigmentary incontinence was observed in 71.88% of the cases and only in 12.5% of the controls on histopathological examination. Overall, it can be suggested that keratinocyte apoptosis leads to melanin incontinence leading to lichen planus-like pigmentation.
Limitations
Relatively small number of controls is the limitation of this study.
Conclusion
Clinical lichen planus-like lesions, although infrequently seen in the oral mucosa of patients with pemphigus, need to be dealt with caution and not ignored as inactive disease or postinflammatory hyperpigmentation. As seen in this study, lichen planus-like lesions in pemphigus have pathology reminiscent of active pemphigus. Thus, these lesions could be harbingers of disease aggravation if treatment is tapered prematurely. In such a situation, clinical examination of the oral mucosa might not be sufficient enough to decide about tapering or withdrawal of medication. A negative direct immunofluorescence report or atleast a routine histopathological examination should be sought in all cases with lichen planus-like lesions without any other lesions clinically characteristic of pemphigus if one considers treatment withdrawal.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patients have given their consent for their images and other clinical information to be reported in the journal. The patients understand that name and initials will not be published and due efforts will be made to conceal identity, but anonymity cannot be guaranteed.
Acknowledgement
Mrs. Sohini Mukherjee for her help in immunohistochemistry.
Financial support and sponsorship
IADVL Research Grant-2015.
Conflicts of interest
There are no conflicts of interest.
| 1. |
Davis EC, Callender VD. Postinflammatory hyperpigmentation: A review of the epidemiology, clinical features, and treatment options in skin of color. J Clin Aesthet Dermatol 2010;3:20-31.
[Google Scholar]
|
| 2. |
Kumar S, De D, Handa S, Ratho RK, Bhandari S, Pal A, et al. Identification of factors associated with treatment refractoriness of oral lesions in pemphigus vulgaris. Br J Dermatol 2017;177:1583-9.
[Google Scholar]
|
| 3. |
Grando SA, Bystryn JC, Chernyavsky AI, Frusić-Zlotkin M, Gniadecki R, Lotti R, et al. Apoptolysis: A novel mechanism of skin blistering in pemphigus vulgaris linking the apoptotic pathways to basal cell shrinkage and suprabasal acantholysis. Exp Dermatol 2009;18:764-70.
[Google Scholar]
|
| 4. |
Pretel M, España A, Marquina M, Pelacho B, López-Picazo JM, López-Zabalza MJ, et al. An imbalance in Akt/mTOR is involved in the apoptotic and acantholytic processes in a mouse model of pemphigus vulgaris. Exp Dermatol 2009;18:771-80.
[Google Scholar]
|
| 5. |
Puviani M, Marconi A, Cozzani E, Pincelli C. Fas ligand in pemphigus sera induces keratinocyte apoptosis through the activation of caspase-8. J Invest Dermatol 2003;120:164-7.
[Google Scholar]
|
| 6. |
Pelacho B, Natal C, España A, Sánchez-Carpintero I, Iraburu MJ, López-Zabalza MJ, et al. Pemphigus vulgaris autoantibodies induce apoptosis in HaCaT keratinocytes. FEBS Lett 2004;566:6-10.
[Google Scholar]
|
| 7. |
Arredondo J, Chernyavsky AI, Karaouni A, Grando SA. Novel mechanisms of target cell death and survival and of therapeutic action of IVIg in pemphigus. Am J Pathol 2005;167:1531-44.
[Google Scholar]
|
| 8. |
Wang X, Brégégère F, Frusić-Zlotkin M, Feinmesser M, Michel B, Milner Y, et al. Possible apoptotic mechanism in epidermal cell acantholysis induced by pemphigus vulgaris autoimmunoglobulins. Apoptosis 2004;9:131-43.
[Google Scholar]
|
| 9. |
Wang X, Brégégère F, Soroka Y, Frusic-Zlotkin M, Milner Y. Replicative senescence enhances apoptosis induced by pemphigus autoimmune antibodies in human keratinocytes. FEBS Lett 2004;567:281-6.
[Google Scholar]
|
| 10. |
Li N, Zhao M, Wang J, Liu Z, Diaz LA. Involvement of the apoptotic mechanism in pemphigus foliaceus autoimmune injury of the skin. J Immunol 2009;182:711-7.
[Google Scholar]
|
| 11. |
Pacheco-Tovar D, López-Luna A, Herrera-Esparza R, Avalos-Díaz E. The caspase pathway as a possible therapeutic target in experimental pemphigus. Autoimmune Dis 2011;2011:563091.
[Google Scholar]
|
| 12. |
Toosi S, Habib N, Torres G, Reynolds SR, Bystryn JC. Serum levels of inhibitors of apoptotic proteins (IAPs) change with IVIg therapy in pemphigus. J Invest Dermatol 2011;131:2327-9.
[Google Scholar]
|
| 13. |
Janse IC, van der Wier G, Jonkman MF, Pas HH, Diercks GF. No evidence of apoptotic cells in pemphigus acantholysis. J Invest Dermatol 2014;134:2039-41.
[Google Scholar]
|
Fulltext Views
4,755
PDF downloads
2,481





![[Figure - 1]](#fig_ijdvl_2020_86_3_278_256906_f1.jpg){kind=link}
![[Table - 1]](#tbl_ijdvl_2020_86_3_278_256906_t5.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2020_86_3_278_256906_f2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2020_86_3_278_256906_f3.jpg){kind=link}
![[Figure - 4]](#fig_ijdvl_2020_86_3_278_256906_f4.jpg){kind=link}