Translate this page into:
High B-cell-activating factor levels in endemic Tunisian pemphigus
2 Department of Dermatology, La Rabta Hospital, Tunis, Tunisia
3 Department of Dermatology, Habib Thameur Hospital, Tunis, Tunisia
4 Department of Dermatology, Charles Nicolle Hospital, Tunis, Tunisia
Correspondence Address:
Maryam Kallel Sellami
Department of Immunology, La Rabta Hospital, Tunis 1007
Tunisia
| How to cite this article: Mejri K, Sellami MK, Zaraa IR, Laadhar L, Lahmar H, Mokni M, Mokhtar I, Fezza B, Zitouni M, Makni S. High B-cell-activating factor levels in endemic Tunisian pemphigus. Indian J Dermatol Venereol Leprol 2017;83:496-499 |
Sir,
B-cell-activating factor belonging to the tumor necrosis factor family plays a crucial role in B-cell development, immunoglobulin production and switch to the IgG, IgE and IgA subclasses. Excessive B-cell-activating factor rescues self-reactive B cells from anergy which may play a crucial role in the induction and development of autoimmunity. Previous reports have shown elevated serum B-cell-activating factor levels in patients with systemic lupus, Sjögren syndrome and rheumatoid arthritis.[1]
Pemphigus is an autoimmune intraepidermal blistering disease characterized by the presence of autoantibodies against desmoglein 1 in pemphigus foliaceus and desmoglein 3 in pemphigus vulgaris. Knowing that B-cell-activating factor pathway is involved in the generation of autoreactive B cells, we analyzed serum B-cell-activating factor levels in Tunisian pemphigus vulgaris and pemphigus foliaceus patients and correlated their levels with clinical presentation and autoantibody profile.[2]
This is a cross-sectional retrospective study on frozen samples at −80°C. Sera were obtained from 50 pemphigus foliaceus patients and 36 pemphigus vulgaris patients with a median age of 44 years (range 17–81). All patients fulfilled clinical and immunological criteria of pemphigus. Forty pemphigus foliaceus patients as well as 29 pemphigus vulgaris patients had recurrent, active disease; the other patients were in remission. Blood sample was collected before corticosteroid treatments in 28 pemphigus foliaceus and 22 pemphigus vulgaris patients. Among pemphigus patients with recurrent, active disease, 9 pemphigus foliaceus and 14 pemphigus vulgaris patients were under systemic therapy at the time of drawing the blood to perform serum B-cell-activating factor measurement. The retrospective nature of the study limited the clinical data concerning severity of the diseases for 27 pemphigus foliaceus and 28 pemphigus vulgaris patients from the case records. For these patients, we evaluated the severity of pemphigus according to the cutaneous and mucosal involvement of defined areas of the body – score 0 (no lesions), score 1 (<25% involvement), score 2 (25%–50%), score 3 (50%–75%) and score 4 (>75%). Thirty eight healthy controls with a median age of 43 years were also recruited in the study.
This investigation was approved by the ethical committee of La Rabta University Hospital. All patients and controls gave their consents for the study.
Pemphigus foliaceus and pemphigus vulgaris patients as well as healthy control were already tested for anti-desmoglein 1 and 3 autoantibodies (MBL, Nagoya, Japan) and the presence of autoantibodies other than anti-desmoglein.[3]
A specific enzyme-linked immunosorbent assay kit was used to measure serum B-cell-activating factor levels (R&D Systems Inc., Minneapolis, USA). Values above the mean ± 2 standard deviation (1168 pg/ml) in control samples were considered as high levels.
Statistical analysis was performed using the Statistical Package for Social Sciences, version 16.0 (SPSS Inc., Chicago, IL, USA). P < 0.05 was considered statistically significant.
In healthy control, serum B-cell-activating factor levels ranged between 200 and 1200 pg/ml with a mean value of 748 ± 206 pg/ml. Serum B-cell-activating factor mean values did not differ between the three groups (pemphigus foliaceus, pemphigus vulgaris and healthy control), yet we note a P value (P = 0.052) near the threshold of significance. However, after Bonferroni correction, serum B-cell-activating factor levels were significantly higher in pemphigus foliaceus patients (mean level 982 ± 557 pg/ml) than in healthy control, P = 0.046. There was no statistically significant difference between pemphigus vulgaris patients and healthy control [Figure - 1].
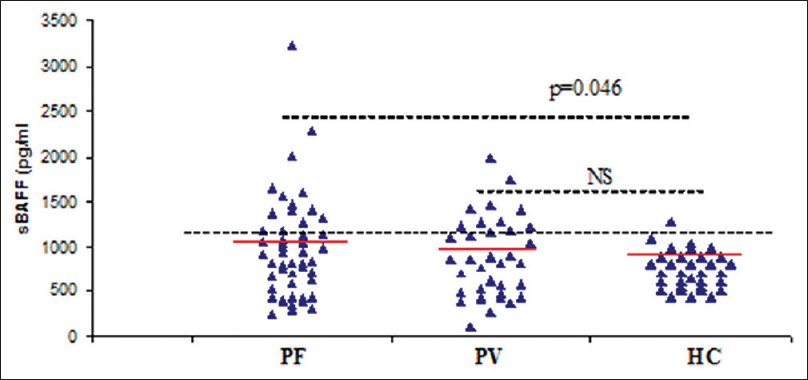 |
| Figure 1: Comparison of serum B-cell-activating factor mean levels (pg/ml) in pemphigus patients (pemphigus foliaceus (PF), pemphigus vulgaris (PV)) and in healthy controls (HC). Significant difference (P < 0.05) was observed with pemphigus foliaceus patients when compared to healthy control (serum B-cell-activating factor means are in red lines). BAFF: B-cell activating factor, NS: Not significant |
High serum B-cell-activating factor levels were observed in 14 (28%) pemphigus foliaceus and 11 (30.5%) pemphigus vulgaris patients.
In pemphigus foliaceus patients, serum B-cell-activating factor levels were significantly higher in those without corticosteroid treatment (mean level 1229 ± 573 pg/ml) than in healthy control (P < 0.001 by t-test). Moreover, mean serum B-cell-activating factor values were significantly higher in patients with high score disease severity (P = 0.012 by t-test) and in those with the recurrent active disease before re-introduction of corticosteroid or any other treatment (P < 0.001 by t-test) [Table - 1].

In pemphigus foliaceus patients, scores for disease severity were available for seven and twenty cases with high and low serum B-cell-activating factor, respectively. Among the seven pemphigus foliaceus patients with high serum B-cell activating factor, all (100%) had widespread disease (score of disease severity 3–4) compared to nine of twenty patients (45%) in those with normal serum B-cell-activating factor (P = 0.02 by Fisher's exact test).
In pemphigus vulgaris patients, scores for disease severity were available for 7 and 21 cases with high and low serum B-cell-activating factor, respectively. Among the seven pemphigus vulgaris patients with high serum B-cell activating factor, only 4 (57%) showed severe lesions compared to 6 of 21 (28%) of those with normal serum B-cell-activating factor.
Although serum B-cell-activating factor levels did not correlate with age, stratification of patients according to the mean age revealed that younger pemphigus foliaceus patients had significantly higher levels.
In both groups, there was no significant correlation between serum B-cell activating factor neither with anti-desmoglein 1/desmoglein 3 autoantibodies titers nor with the presence of autoantibodies other than anti-desmoglein.
Unlike previous studies, our findings revealed the presence of a significant difference among autoimmune pemphigus patients and controls.[2],[4]
Matsushita et al. did not find a significant difference between pemphigus or pemphigoid patients and the control group regarding serum B-cell-activating factor levels.[2] Asashima et al. reported a significant difference in bullous pemphigoid, but not in pemphigus vulgaris patients.[4] In this study, we found that serum B-cell activating factor values were significantly higher in pemphigus foliaceus patients than in healthy control. Interestingly, significant associations between serum B-cell-activating factor values, younger age and clinical status (absence of corticosteroid treatment and disease activity) were found only in the pemphigus foliaceus group. In Tunisia, pemphigus has particular epidemiological features: pemphigus foliaceus is the endemic form of the disease; it is predominantly observed in women of the reproductive age group. These patients have common human leukocyte antigen susceptibility alleles which vary from the ones observed in the sporadic form in the north of the country.[5] Thus, B-cell activating factor elevation occurs mainly in patients with Tunisian endemic pemphigus features.
Serum B-cell activating factor mean levels were found to be significantly lower in patients under corticosteroid treatment. This effect is different from that seen in rituximab-treated patients.[6] In this study, we failed to find a significant correlation between anti-desmoglein 1/desmoglein 3 autoantibodies titers and serum B-cell-activating factor, while in systemic lupus erythematosus, a strong association was found between anti-deoxyribonucleic acid antibodies titers and serum B-cell-activating factor values. Moreover, serum B-cell-activating factor levels in Tunisian systemic lupus erythematosus cases are significantly higher compared to those found in Tunisian pemphigus foliaceus patients (2340.72 ± 1000 pg/ml, unpublished data).
The presence of high levels of serum B-cell-activating factor suggests that this cytokine induces the expansion of activated B and T cells and autoantibodies production. This overexpression, significantly observed in the absence of treatment mainly on the earlier onset of pemphigus foliaceus, suggests that serum B-cell-activating factor participated in the proliferation of autoreactive cells, thus enhancing the autoimmune response. Besides, it has been reported that B-cell-activating factor acts on dendritic cells helping them to increase the pro-inflammatory activity of T cells. This is in accordance with the association of high serum B-cell-activating factor levels with high score disease in pemphigus foliaceus. This data may reflect serum B-cell-activating factor contributing to pemphigus pathogenesis.
Interestingly, B-cell-activating factor polymorphism −871C/T is involved in pemphigus foliaceus pathogenesis.[7] Analyzing the association of this polymorphism in our patients and assessing its functional impact are needed to investigate the biological significance of serum B-cell-activating factor elevation in pemphigus foliaceus patients. Targeting B-cell-activating factor with monoclonal antibodies (belimumab) has been approved for systemic lupus erythematosus treatment, but clinical and theoretical arguments for a potential beneficial effect in pemphigus are lacking.[8]
In conclusion, we described the presence of higher levels of serum B-cell-activating factor in pemphigus foliaceus patients. These levels correlated with disease activity in patients without treatment. Because this finding is mainly observed in patients with features of the endemic form of Tunisian pemphigus foliaceus, it needs to be confirmed in other endemic forms of pemphigus within homogeneous and comparable age repartition and disease duration. Answering this question will clarify whether the autoimmune mechanisms through serum B-cell-activating factor varies among pemphigus forms and possibly making the endemic forms distinct.
Acknowledgment
This work was supported by research grant from University of Tunis El Manar to “Immuno-Rheumatology laboratory “ La Rabta Hospital, 1007 Tunis, Tunisia.
Financial support and sponsorship
The study was supported by grants by from Tunis El Manar University, The Tunisian ministry of higher education and scientific research (LR05SP01).
Conflicts of interest
There are no conflicts of interest.
| 1. |
Moisini I, Davidson A. BAFF: A local and systemic target in autoimmune diseases. Clin Exp Immunol 2009;158:155-63.
[Google Scholar]
|
| 2. |
Matsushita T, Hasegawa M, Matsushita Y, Echigo T, Wayaku T, Horikawa M, et al. Elevated serum BAFF levels in patients with localized scleroderma in contrast to other organ-specific autoimmune diseases. Exp Dermatol 2007;16:87-93.
[Google Scholar]
|
| 3. |
Mejri K, Abida O, Kallel-Sellami M, Haddouk S, Laadhar L, Zarraa IR, et al. Spectrum of autoantibodies other than anti-desmoglein in pemphigus patients. J Eur Acad Dermatol Venereol 2011;25:774-81.
[Google Scholar]
|
| 4. |
Asashima N, Fujimoto M, Watanabe R, Nakashima H, Yazawa N, Okochi H, et al. Serum levels of BAFF are increased in bullous pemphigoid but not in pemphigus vulgaris. Br J Dermatol 2006;155:330-6.
[Google Scholar]
|
| 5. |
Abida O, Zitouni M, Kallel-Sellami M, Mahfoudh N, Kammoun A, Ben Ayed M, et al. Tunisian endemic pemphigus foliaceus is associated with the HLA-DR3 gene: Anti-desmoglein 1 antibody-positive healthy subjects bear protective alleles. Br J Dermatol 2009;161:522-7.
[Google Scholar]
|
| 6. |
Nagel A, Podstawa E, Eickmann M, Müller HH, Hertl M, Eming R. Rituximab mediates a strong elevation of B-cell-activating factor associated with increased pathogen-specific IgG but not autoantibodies in pemphigus vulgaris. J Invest Dermatol 2009;129:2202-10.
[Google Scholar]
|
| 7. |
Malheiros D, Petzl-Erler ML. Individual and epistatic effects of genetic polymorphisms of B-cell co-stimulatory molecules on susceptibility to pemphigus foliaceus. Genes Immun 2009;10:547-58.
[Google Scholar]
|
| 8. |
Mahieu MA, Strand V, Simon LS, Lipsky PE, Ramsey-Goldman R. A critical review of clinical trials in systemic lupus erythematosus. Lupus 2016;25:1122-40.
[Google Scholar]
|
Fulltext Views
1,460
PDF downloads
913





![[Figure - 1]](#fig_ijdvl_2017_83_4_496_206725_f1.jpg){kind=link}
![[Table - 1]](#tbl_ijdvl_2017_83_4_496_206725_t2.jpg){kind=link}