Translate this page into:
Atypical cutaneous features in adult onset Still's disease
2 Department of Physical Therapy and Rehabilitation, Dicle University Faculty of Medicine, Turkey
3 Department of Pathology, Dicle University Faculty of Medicine, Turkey
Correspondence Address:
Zeynep Meltem Akkurt
Department of Dermatology, Dicle University Faculty of Medicine, Diyarbakir
Turkey
| How to cite this article: Akkurt ZM, Bozkurt M, U�mak D, T�rkc� G, U�ak H. Atypical cutaneous features in adult onset Still's disease. Indian J Dermatol Venereol Leprol 2014;80:250-253 |
Abstract
Adult onset Still's disease is a rare but potentially serious disease. We present five cases of adult-onset Still's disease seen by us over a period of one year. The patients were all females and 28-39 years of age. Symptoms had been present for 2-6 weeks in three patients. The other two had been on a few years' follow-up for rheumatoid arthritis before the onset of rashes and fever. The patients had persistent erythematous maculopapular eruptions on face, body and extremities, with moderate to severe pruritus and/or a burning sensation that decreased their quality of life. The typical evanescent rash was not observed. High ferritin values were detected in all the patients and total serum IgE was increased in two. All the patients were started on oral prednisolone (0.5-1.0 mg/kg/day), and methotrexate (10-15 mg/week) had to be added in three patients. One patient was started on tocilizumab due to recalcitrant disease and one was lost to follow-up. Further investigation and classification of the various atypical cutaneous findings in adult-onset Still's disease is necessary.INTRODUCTION
Adult-onset Still′s disease is a rare and potentially crippling disease, which may be fatal in young adults. [1],[2] The clinical picture overlaps with that of many other conditions in the general population such as infections, drug eruptions and collagen vascular diseases. [3] It is slightly more common in females than in males. [1] The occurrence of an evanescent rash is generally considered a major diagnostic criterion. [4] Other kinds of rashes are not included in the guidelines and are therefore not considered to be of diagnostic significance. [3] Recent studies have however increasingly reported atypical skin rashes in patients with adult-onset Still′s disease.
Case Report
Five female patients presented with atypical rashes to the Rheumatology Department of Diyarbakir University Hospital over a one-year period, out of a total of 15 patients diagnosed with adult-onset Still′s disease. The patients′ ages ranged from 28 to 39 years. The duration of symptoms was 2-6 weeks in three patients. Two patients had been followed up with a diagnosis of rheumatoid arthritis for a few years before the onset of rashes and fever. All five patients were diagnosed to have adult-onset Still′s disease since they met five criteria, including a minimum of two major criteria, as described by Yamaguchi et al. [4] The major criteria are: Fever of >39°C lasting for at least one week, arthralgias lasting for at least two weeks, a non-pruritic salmon-colored rash, and leukocytosis; the minor criteria are: Sore throat, lymphadenopathy, hepatomegaly or splenomegaly, abnormal liver function tests, and negative antinuclear antibody and rheumatoid factor tests. Further, we used the American Rheumatism Association criteria to rule out other rheumatic diseases such as systemic lupus erythematosus. Repeated blood cultures and serological tests for brucellosis were negative; neoplastic conditions were also ruled out. Serum ferritin levels ranged from 5388 to 16518 ng/mL. Total serum IgE was measured in two patients and found to be 3640 IU/mL and 199 IU/mL, respectively. The clinical features and significant laboratory test results are summarized in [Table - 1].

The patients had pinkish, erythematous maculo-papular eruptions spread on the face, trunk and extremities. The lesions occurred along with fever and arthralgia in the span of a week. Three patients had edema, particularly on the face. All patients complained of moderate to severe pruritus and/or a burning sensation which significantly reduced the quality of life. None of the patients had the typical evanescent rashes of adult-onset Still′s disease.
Patient 1 had widespread erythematous pigmented plaques with a linear pattern and follicular accentuation [Figure - 1]a, while patient 2 had localized papules and plaques, which demonstrated follicular accentuation [Figure - 1]b. Patients 3-5 had widespread confluent edematous papular eruptions [Figure - 2]a and b]. Three of the patients consented to skin biopsy. Histopathological examination showed a mixed inflammatory infiltrate in the upper dermis, and one biopsy had necrotic keratinocytes in the epidermis [Figure - 3].
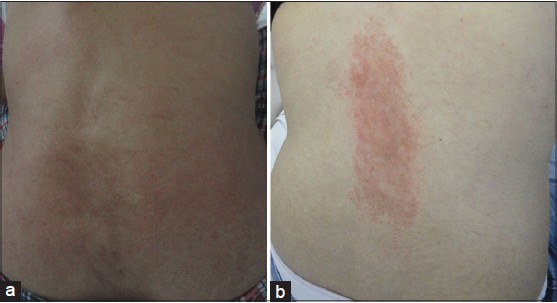 |
| Figure 1: (a) Widespread erythematous pigmented plaques with linear and follicular accentuation, (b) Localized plaques with follicular accentuation |
 |
| Figure 2: (a and b) Widespread confluent and edematous maculopapular eruption |
 |
| Figure 3: Necrotic keratinocytes (arrows) in the upper portion of a slightly acanthotic epidermis (H and E, ×100) |
Topical corticosteroids and systemic antihistamines did not relieve the pruritus and burning sensation and all patients required treatment with oral prednisolone at a dose of 0.5-1.0 mg/kg/day. One patient was subsequently lost to follow-up. Three patients were also administered methotrexate at a dose of 10-15 mg/week in combination with prednisolone. The rashes improved in a few weeks, and complete remission was achieved in 2-3 months in four patients. Patient 4 however did not respond to this treatment and was put on tocilizumab, with which partial remission was achieved in a month. Patient 2 had a recurrence of rashes and pruritus along with fever and arthralgia on stopping treatment.
DISCUSSION
Adult-onset Still′s disease was first described by Bywaters in 14 patients, all of whom had evanescent small salmon-pink macules which rarely itched [5] but recent reports have increasingly described patients with atypical eruptions, mostly persistent or fixed papules and/or plaques. [6],[7],[8],[9] Urticaria has also been reported. [3],[10] Pruritic eruptions with linear lesions, as in one of our patients, have been reported as well, being described as dermographism by some authors [10] and a Koebner phenomenon by others. [11] Lee et al., have termed all atypical eruptions "persistent pruritic eruptions" and classified them clinically as urticarial papules, lichenoid papules, dermographism-like lesions, dermatomyositis-like lesions, prurigo pigmentosa-like lesions and lichen amyloidosus-like lesions. They suggest that these variants may all be manifestations of a single process progressing from urticarial papules and plaques to lichenoid papulosquamous lesions. They also note the tendency to seasonal variation among their patients, who first presented during spring and autumn. [12]
Histopathologically, numerous single or multiple necrotic keratinocytes in the upper half of the epidermis with a neutrophilic and lymphocytic infiltrate in the upper dermis are typical. In addition, a marked lack of eosinophils is distinctive. [7],[12] Serum IgE was notably elevated in 2 of our patients but the significance of this finding is unclear. We recommend that levels of IgE be assessed in all patients with adult-onset Still′s disease.
The frequency of atypical eruptions among patients with adult-onset Still′s disease has been reported to be 29-78%. [7],[12],[13] Although the typical rash has a relatively high sensitivity and specificity, some forms of atypical rashes may have prognostic significance. For instance, persistent plaques, linear pigmentation and dermatomyositis-like eruptions have been associated with a more severe clinical course [12],[14] and suggested to be a clinical marker of disease severity. [6],[9] Such cutaneous manifestations may therefore be an indication for the institution of more aggresive systemic treatments. In conclusion, atypical cutaneous features seem to be more frequent than expected among patients with adult-onset Still′s disease. They may help in establishing the correct diagnosis and also in assessing disease severity and response to therapy.
| 1. |
Colina M, Zucchini W, Ciancio G, Orzincolo C, Trotta F, Govoni M. The evolution of adult-onset still disease: An observational and comparative study in a cohort of 76 Italian patients. Semin Arthritis Rheum 2011;41:279-85.
[Google Scholar]
|
| 2. |
Yokoi K, Hosoi E, Nakanishi M, Goto T, Saito S. Increased serum IgE level and interleukin-4 release from cultured lymphocytes from a patient with adult onset Still's disease. Ann Rheum Dis 1995;54:752-3.
[Google Scholar]
|
| 3. |
Affleck AG, Littlewood SM. Adult-onset Still's disease with atypical cutaneous features. J Eur Acad Dermatol Venereol 2005;19:360-3.
[Google Scholar]
|
| 4. |
Yamaguchi M, Ohta A, Tsunematsu T, Kasukawa R, Mizushima Y, Kashiwagi H, et al. Preliminary criteria for classification of adult Still's disease. J Rheumatol 1992;19:424-30.
[Google Scholar]
|
| 5. |
Bywaters EG. Still's disease in the adult. Ann Rheum Dis 1971;30:121-33.
[Google Scholar]
|
| 6. |
Suzuki K, Kimura Y, Aoki M, Takezaki S, Tuchida T, Takano T, et al. Persistent plaques and linear pigmentation in adult-onset Still's disease. Dermatology 2001;202:333-5.
[Google Scholar]
|
| 7. |
Lee JY, Yang CC, Hsu MM. Histopathology of persistent papules and plaques in adult-onset Still's disease. J Am Acad Dermatol 2005;52:1003-8.
[Google Scholar]
|
| 8. |
Tomaru K, Nagai Y, Ohyama N, Hasegawa M, Endo Y, Tamura A, et al. Adult-onset Still's disease with prurigo pigmentosa-like skin eruption. J Dermatol 2006;1:5-8.
[Google Scholar]
|
| 9. |
Lübbe J, Hofer M, Chavaz P, Saurat JH, Borradori L. Adult-onset Still's disease with persistent plaques. Br J Dermatol 1999;141:710-3.
[Google Scholar]
|
| 10. |
Criado PR, de Carvalho JF, Ayabe LA, Brandt HR, Romiti R, Maruta CW. Urticaria and dermographism in patients with adult-onset Still's disease. Rheumatol Int 2012;32:2551-5.
[Google Scholar]
|
| 11. |
Yamamoto T. Cutaneous manifestations associated with adult-onset Still's disease: Important diagnostic values. Rheumatol Int 2012;32:2233-7.
[Google Scholar]
|
| 12. |
Lee JY, Hsu CK, Liu MF, Chao SC. Evanescent and persistent pruritic eruptions of adult-onset still disease: A clinical and pathologic study of 36 patients. Semin Arthritis Rheum 2012;42:317-26.
[Google Scholar]
|
| 13. |
Nagai Y, Hasegawa M, Okada E, Hattori T, Tago O, Ishikawa O. Clinical follow-up study of adult-onset Still's disease. J Dermatol 2012;39:898-901.
[Google Scholar]
|
| 14. |
Ohashi M, Moriya C, Kanoh H, Kinomura Y, Terakura Y, Kasahara S, et al. Adult-onset Still's disease with dermatomyositis-like eruption. J Dermatol 2012;39:958-60.
[Google Scholar]
|
Fulltext Views
2,586
PDF downloads
1,214





![[Table - 1]](#tbl_ijdvl_2014_80_3_250_132254_b2.jpg){kind=link}
![[Figure - 1]](#fig_ijdvl_2014_80_3_250_132254_u1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2014_80_3_250_132254_u3.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2014_80_3_250_132254_u4.jpg){kind=link}