Translate this page into:
Bowen's disease on finger: A diagnostic and therapeutic challenge
2 Department of Pathology,All India Institute of Medical Sciences (AIIMS), New Delhi, India
3 Department of Surgery, All India Institute of Medical Sciences (AIIMS), New Delhi, India
Correspondence Address:
Binod K Khaitan
Additional Professor, Department of Dermatology, Venereology, and Leprology,All India Institute of Medical Sciences (AIIMS)New Delhi-110029
India
| How to cite this article: Singh S, Khaitan BK, Sharma MC, Seenu V, Kumawat M, Chatterjee P. Bowen's disease on finger: A diagnostic and therapeutic challenge. Indian J Dermatol Venereol Leprol 2013;79:227-230 |
Abstract
Bowen's disease commonly presents as a solitary asymptomatic plaque involving head and neck region or lower limbs. We present a case of a sixty seven-year-old man with an itchy, oozy, crusted solitary plaque on the right ring finger of eighteen months duration with histopathology consistent with Bowen's disease. The lesion was initially treated with topical 5% imiquimod but due to relapse and inadequate response to a second course, complete surgical excision followed by full thickness skin grafting was done. Recurrence after about 6 months in the form of a small papule adjacent to the initial site was also treated with excision. This report highlights the potential of Bowen's disease to mimic more common dermatoses and a high index of suspicion, supported by histopathology, is required to diagnose and treat it without delay, which in turn may require a multimodality approach. We also reviewed the current literature on the same.Introduction
Bowen′s disease is an intraepithelial carcinoma or squamous cell carcinoma in-situ of the epidermis. It can be found on both sun exposed and unexposed areas; head and neck and lower limbs being the common sites. [1] Although several treatment modalities are available for Bowen′s disease, no single therapy has been proven to be superior to others. [2] Imiquimod is a topical immune response modifier which has been widely used by dermatologists successfully in treating Bowen′s disease, actinic keratosis, superficial basal cell carcinoma and even invasive squamous cell carcinomas. [1],[3],[4],[5] We describe an unusual case of Bowen′s disease presenting as a single dermatitic plaque on finger which recurred despite adequate therapy with imiquimod.
Case Report
A sixty seven-year-old elderly man presented with a single erythematous plaque on side of right ring finger for eighteen months. The lesion initially started as a tiny asymptomatic erythematous papule few weeks apparently following a minor blunt injury at the site. The lesion gradually enlarged to form a plaque associated with moderate pruritus and occasional clear ooze. Before presenting to us, he had been treated with topical steroid antibiotic combinations for few weeks and systemic antibiotics without any improvement. Dermatological examination showed a single 3 × 2cm round to oval well defined erythematous plaque on the lateral aspect of the right ring finger which was covered with thick semi adherent yellowish-black crust, removal of which showed a non-indurated erythematous mildly oozy base without frank bleeding [Figure - 1]a. There were no loco-regional lymphadenopathy or skin lesions elsewhere. Keeping the provisional possibilities of fixed cutaneous sporotrichosis, tuberculosis verrucosa cutis and chromoblastomycosis, a skin biopsy was performed using a 4 mm punch from the plaque which showed epidermal hyperkeratosis, irregular acanthosis with many dyskeratotic cells, mitotic figures and keratinocyte dysplasia and atypia. Dermis showed perivascular lympho-histiocytic infiltrate in upper part without any invasion. These histological features were consistent with squamous cell carcinoma in situ Bowen′s disease [Figure - 1]b and c. Therefore, a revised diagnosis of Bowen′s disease was made and the patient was started on topical-imiquimod 5% cream 6 days a week. The patient took therapy regularly for thirteen weeks (followed up clinically till 9 weeks showing few persistent papules, [Figure - 2], beyond which he stopped it on his own due to complete subsidence of the lesion. Seven months after stopping treatment, patient reported back with complaint of few papules at the same site [Figure - 3]a from which a repeat biopsy again showed features of Bowen′s disease. Patient was restarted on topical imiquimod therapy in the same fashion as before and this time for sixteen weeks. Because of persistence and progression of disease despite above treatment [Figure - 3]b, a more radical approach was followed and the lesion was completely excised with 1 mm margin and the defect repaired with full thickness skin graft taken from the opposing side of the adjacent middle finger. Patient was alright for 6 months but reported back with presence of a tiny keratotic papule adjacent to the grafted area, which was excised with 1 mm margin and histology showed features of Bowen′s disease, but margins were free of the tumor. Patient has been recurrence free for the past eleven months and the grafted skin and adjacent areas are healthy [Figure - 3]c.
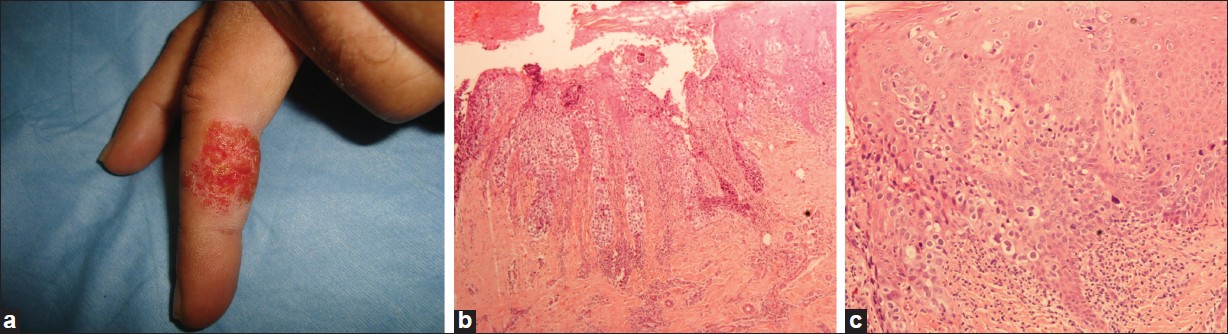 |
| Figure 1: (a) The erythematous plaque (at baseline) on right ring finger after crust removal; (b) Histopathology of punch biopsy from the plaque. (1) Low power view showing the hyperkeratosis, irregular acanthosis and full thickness dysplasia of the epidermis (H and E, x 40) (2) Close up view of the same showing epidermis with cellular hyperchromatia, atypia, dyskeratosis and mitosis with intact basal lamina (H and E, x 100) |
 |
| Figure 2: Plaque after 9 weeks of topical imiquimod application showing nearly complete resolution |
 |
| Figure 3: Follow up photographs. (a) Showing persistent scaly papules at 7 months after completing 1st course of 13 weeks imiquimod application. (b) Lesion after completing 2nd course of 16 weeks imiquimod application (c) Status at 11 months after the 2nd excision, 16 months after the 1st excision (5 months after the 1st excision and skin grafting, a 2nd elliptical excision was done for a minor relapse outside the grafted area |
Discussion
Bowen′s disease is an intraepithelial squamous cell carcinoma first described by John Bowen in 1912. It usually occurs as a solitary plaque which is often asymptomatic but multiple lesions can occur in 10- 20% of the cases. [2] Our case was unusual for several reasons. First, the morphology of the lesion in the form of a solitary itchy, erythematous, dermatitic plaque was atypical. Bowen′s disease generally presents as an erythematous, irregular, scaly plaque. The well established clinical variants include pigmented, subungual/periungual, palmar, genital and perianal and verrucous Bowen′s disease, [2] and it has also been reported to mimic malignant melanoma. [6] As far as ascertained, there is a single report of Bowen′s disease in English literature of an eczematous plaque involving distal digit. [7]
Secondly, the location of the lesion over the finger was also atypical. The common sites for Bowen′s disease include the chronically photo-exposed sites like head and neck and dorsae of hands and lower legs. [1],[2] There have been few studies with large cohorts, [8],[9],[10] analyzing the site distribution of Bowen′s disease. Thestrup-Pedersen et al. [8] described six hundred seventeen cases of Bowen′s disease out of which 73.5% cases occurred over photo-exposed sites (head and neck, and hands). Kossard et al.[9] analyzed data of one thousand one histologically proven cases of Bowen′s disease and found head and neck region to be the commonest site (44%) followed by lower limb (29.8%), upper limb (19.8%) and torso (6.5%). On the other hand, in the series of one hundred eight cases by Cox, [10] lower limbs were the commonest sites (75%), followed by face and scalp (13%) and hands and wrists (11%). But none of these studies give any details about digital lesions. Although anecdotal reports of Bowen′s disease occurring over digits have been described, [7],[11],[12],[13] it still remains a rare site.
On histology, our patient showed scattering of atypical cells (with abundant cytoplasm) within the adjacent epidermis alongside the zone of full thickness dysplasia. This suggests pagetoid pattern in Bowen′s disease. This is a rare variant, its incidence being reported as 5% among all cutaneous Bowen′s biopsies done at a single institution. [14] Other entities which show such pagetoid histomorphology include extra mammary paget′s disease, pagetoid melanoma in situ, clonal seborrheic keratosis, pagetoid spitz nevus, merkel cell carcinoma with intra-epidermal pagetoid spread, mycosis fungoides and some other rarer disorders. [15] Extra mammary paget′s disease (EPD) and pagetoid melanoma in situ (MIS) represent close histological differentials which, can be conclusively differentiated only on the basis of immunohistochemistry. The same could not be performed in our case, but there were several clues on histology which favoured Bowen′s disease like presence of full thickness dysplasia in majority of the section, presence of atypical pagetoid cells at all levels of the epidermis, scattered multinucleated tumor giant cells, intactness of intercellular bridges between pagetoid cells, lack of involvement of adnexal epithelium by the atypical cells, presence of dyskeratotic keratinocytes and presence of cytoplasmic keratohyaline granules in some of the cells. On the other hand, EPD shows large pale cells (paget cells) in the epidermis, lack of intercellular bridges between the paget cells, nests of atypical cells primarily within the lower layers of the epidermis, tendency to involve the adnexal epithelium and sometimes associated with signet ring cells. In pagetoid MIS, nests of atypical cells are usually located at the dermo-epidermal junction, often containing fine cytoplasmic melanin, with extension of atypical cells both higher up in the stratum corneum as well as, into the follicular epithelium. [16],[17]
Treatment options for Bowen′s disease include cryotherapy, curettage with cautery, excision, topical 5-fluorouracil (5-FU), topical imiquimod, radiotherapy, CO 2 laser, photodynamic therapy (PDT) and topical diclofenac. [18] In our clinical practice we have previously used imiquimod as first line therapy in several patients with solitary/few lesions at extra-digital sites with satisfactory results (unpublished). The response to topical imiquimod was unsatisfactory in the present case as the lesion, though responded well initially but recurred later even after two courses of thirteen and sixteen weeks, respectively. We opted for complete surgical excision with full thickness skin flap. The current literature supports our approach of surgery as there are 3 reports/series on failure of imiquimod for cutaneous Bowen′s. Gong et al.[7] described a case of eczematous plaque over distal part of finger (histologically Bowen′s) which resolved initially with sixteen week imiquimod therapy only to recur after 2 months when the same regimen was repeated. But the lesion was nonresponsive the second time and was invading the underlying bone, thus prompting ray amputation of the finger. The histological evaluation of the excised specimen revealed invasive squamous cell carcinoma (SCC) invading the bone. Similarly, Goh [19] and Murphy et al.[20] have described cases in which Bowen′s disease initially responded to imiquimod but recurred as SCCs which were treated with complete excision without recurrence.
As of now, there are no standard guidelines on the management of digital Bowen′s disease probably due to relative rarity of the condition. The current British Academy of Dermatologists (BAD) guidelines, [2] (2006) mention that for digital Bowen′s, excision may be a better option than all other modalities and that micrographic surgery may be considered for tissue sparing or for poorly defined or recurrent lesions. It also adds that cryotherapy, radiotherapy, PDT, laser and topical 5-FU are all fair options. For topical imiquimod, however, there is insufficient evidence to recommend use in digital lesions.
All therapeutic options have failures and recurrence rates at least in the order of 5-10%, and no treatment modality appears to be superior for all clinical situations. [2] Hence, a follow-up for possible recurrence at 6-12 months is recommended, [2] although few authors recommend that gold standard for cure rate in skin cancers (as for other cancers) should be 5 year-point after treatment. [20] A more practical approach is to follow such patients for at least 1 year post-treatment to detect a recurrence.
| 1. |
Duncan KO, Geisse JK, Leffell DJ. Epithelial precancerous lesions. In: Wolff K, Goldsmith LA, Katz SI, Gilchrest BA, Paller BS, Leffell DJ, editors. Fitzpatrick's Dermatology in General Medicine, 7 th ed. New York: Mcgraw-Hill; 2008. p. 1007-27.
th ed. New York: Mcgraw-Hill; 2008. p. 1007-27.'>[Google Scholar]
|
| 2. |
Cox NH, Eedy DJ, Morton CA. Guidelines for management of Bowen's disease: 2006 update. Br J Dermatol 2007;156:11-21.
[Google Scholar]
|
| 3. |
Peris K, Micantonio T, Fargnoli MC, Lozzi GP, Chimenti S. Imiquimod 5% cream in the treatment of Bowen's disease and invasive squamous cell carcinoma. J Am Acad Dermatol 2006;55:324-7.
[Google Scholar]
|
| 4. |
Warshauer E, Warshauer BL. Clearance of basal cell and superficial squamous cell carcinomas after imiquimod therapy. J Drugs Dermatol 2008;7:447-51.
[Google Scholar]
|
| 5. |
Korman N, Moy R, Ling M, Matheson R, Smith S, McKane S et al.0 Dosing with 5% imiquimod cream 3 times per week for the treatment of actinic keratosis: Results of two phase 3, randomized, double-blind, parallel-group, vehicle-controlled trials. Arch Dermatol 2005;141:467-73.
[Google Scholar]
|
| 6. |
Firooz A, Farsi N, Rashighi-Firoozabadi M, Gorouhi F. Pigmented Bowen's disease of the finger mimicking malignant melanoma. Arch Iran Med 2007;10:255-7.
[Google Scholar]
|
| 7. |
Gong HS, Cho JH, Roh YH, Chung MS, Baek GH. Bone invasion by squamous cell carcinoma in situ (Bowen's disease) of the finger during treatment with imiquimod 5% cream: Case report. J Hand Surg Am 2010;35:999-1002.
[Google Scholar]
|
| 8. |
Thestrup-Pedersen K, Ravnborg L, Reymann F. A description of disease in 617 patients. Acta Derm Venereol 1988;68:236-9.
[Google Scholar]
|
| 9. |
Kossard S, Rosen R. Cutaneous Bowen's disease: An analysis of 1001 cases according to age, sex and site. J Am Acad Dermatol 1992;27:406-10.
[Google Scholar]
|
| 10. |
Cox NH. Body site distribution of Bowen's disease. Br J Dermatol 1994;130:714-6.
[Google Scholar]
|
| 11. |
Gordon KB, Garden JM, Robinson JK. Bowen's disease of the distal digit: Outcome of treatment with carbon dioxide laser vaporization. Dermatol Surg 1996;22:723-8.
[Google Scholar]
|
| 12. |
Wong TW, Sheu HM, Lee JY, Fletcher RJ. Photodynamic therapy for Bowen's disease (squamous cell carcinoma in situ) of the digit. Dermatol Surg 2001;27:452-6.
[Google Scholar]
|
| 13. |
Souza CS, Felício LB, Bentley MV, Tedesco AC, Ferreira J, Kurachi C, et al. Topical photodynamic therapy for Bowen's disease of the digit in epidermolysis bullosa. Br J Dermatol 2005;153:672-4.
[Google Scholar]
|
| 14. |
Strayer DS, Santa Cruz DJ. Carcinoma in situ of the skin: A review of histopathology. J Cutan Pathol1980;7:244-59.
[Google Scholar]
|
| 15. |
Fitzpatrick JE. The histologic diagnosis of intraepithelial pagetoid neoplasms. Clin Dermatol 1991;9:255-9.
[Google Scholar]
|
| 16. |
Bayer-Garner IB, Reed JA. Immunolabeling pattern of syndecan-1 expression may distinguish pagetoid Bowen's disease, extramammary Paget's disease and pagetoid malignant melanoma in situ. J Cutan Pathol 2004;31:169-73.
[Google Scholar]
|
| 17. |
Raju RR, Goldblum JR, Hart WR. Pagetoid squamous cell carcinoma in situ (pagetoid Bowen's disease) of the external genitalia. Int J Gynecol Pathol 2003;22:127-35.
[Google Scholar]
|
| 18. |
Neubert T, Lehmann P. Bowen's disease- A review of newer treatment options. Ther Clin Risk Manag 2008;4:1085-95.
[Google Scholar]
|
| 19. |
Goh MS. Invasive squamous cell carcinoma after treatment of carcinoma in situ with 5% imiquimod cream. Australas J Dermatol 2006;47:186-8.
[Google Scholar]
|
| 20. |
Murphy ME, Brodland DG, Zitelli JA. Definitive surgical treatment of 24 skin cancers not cured by prior imiquimod therapy: A case series. Dermatol Surg 2008;34:1258-63.
[Google Scholar]
|
Fulltext Views
3,237
PDF downloads
393





![[Figure - 1]](#fig_ijdvl_2013_79_2_227_107643_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2013_79_2_227_107643_f2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2013_79_2_227_107643_f3.jpg){kind=link}