Translate this page into:
Store and forward teledermatology
2 Department of Skin and Sexually Transmitted Diseases, PSG Medical College Hospitals, Peelamedu, Coimbatore, Tamil Nadu, India
Correspondence Address:
Garehatty Rudrappa Kanthraj
"Sri Mallikarjuna Nilaya", # HIG 33 Group 1 Phase 2, Hootagally KHB Extension, Mysore - 570018, Karnataka
India
| How to cite this article: Kanthraj GR, Srinivas CR. Store and forward teledermatology. Indian J Dermatol Venereol Leprol 2007;73:5-12 |
Abstract
Store and forward and real time or videoconferences are the two types of teledermatology services practiced. Dermatology and radio-diagnosis are visual specialties suited for store-and-forward teledermatology (SAFT). Advances in information technology, electronic instruments and biotechnology have revolutionized and brought changes in SAFT. Cellular phone, digital camera, personal digital assistants, Wi-Fi, Wi-Max and computer- aided-design software are incorporated to deliver the quality health care to remote geographic regions. Complete SAFT care equivalent to face-to-face consultation (Gold standard) is essential. Health care providers in rural areas are the 'eyes' for the consultants. Consultants to guide them should have a rapid periodic audit of visual parameters and dimensions of lesions. Given this background, this article reviews advances in 1) capture, store and transfer of images. 2) Computer Aided measurements of generalized and localized lesions and 3) the integration model to meet all the above two requirements in a centralized location. This process enables diagnosis, management, periodic assessment and complete follow-up care to achieve patient and physician satisfaction. Preservation of privacy and confidentiality of digital images is important. Uniform rules and regulations are required. Indian space research organization (ISRO), Government of India has demonstrated telemedicine pilot projects utilizing the satellite communication and mobile telemedicine units to be useful in meeting the health care needs of remote and rural India. we have to join hands with them to meet dermatology problems in rural areas.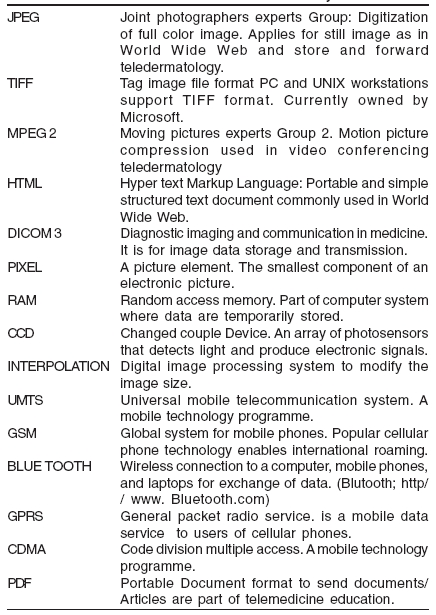
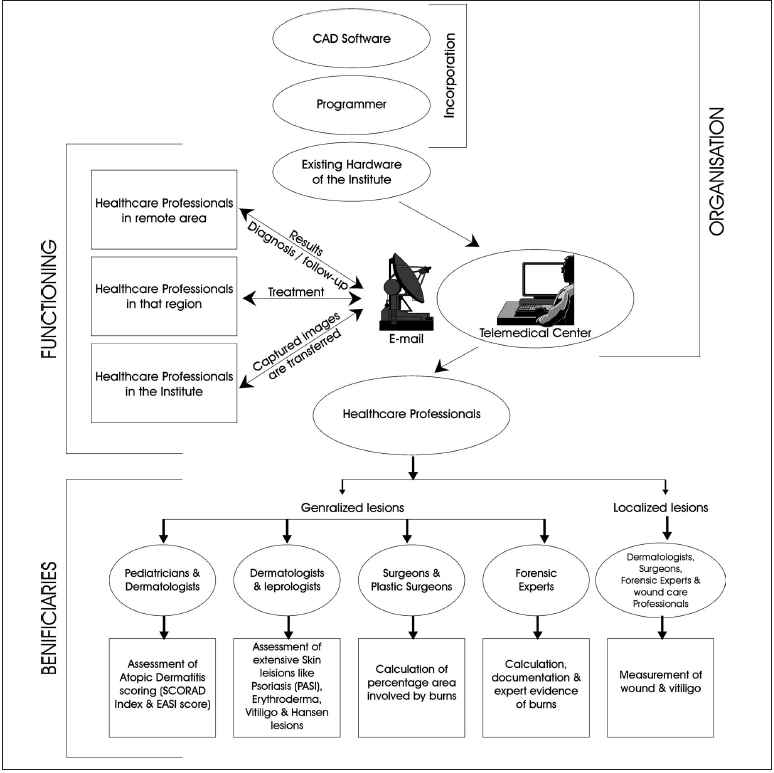 |
| Organization, functioning and beneficiaries of a store-and-forward telemedical center. Modified with permission Kanthraj GR. Pediatr Allergy Immunol 2005;16:182-183. . Blackwell publishers, Oxford, UK |
|
| Organization, functioning and beneficiaries of a store-and-forward telemedical center. Modified with permission Kanthraj GR. Pediatr Allergy Immunol 2005;16:182-183. . Blackwell publishers, Oxford, UK |
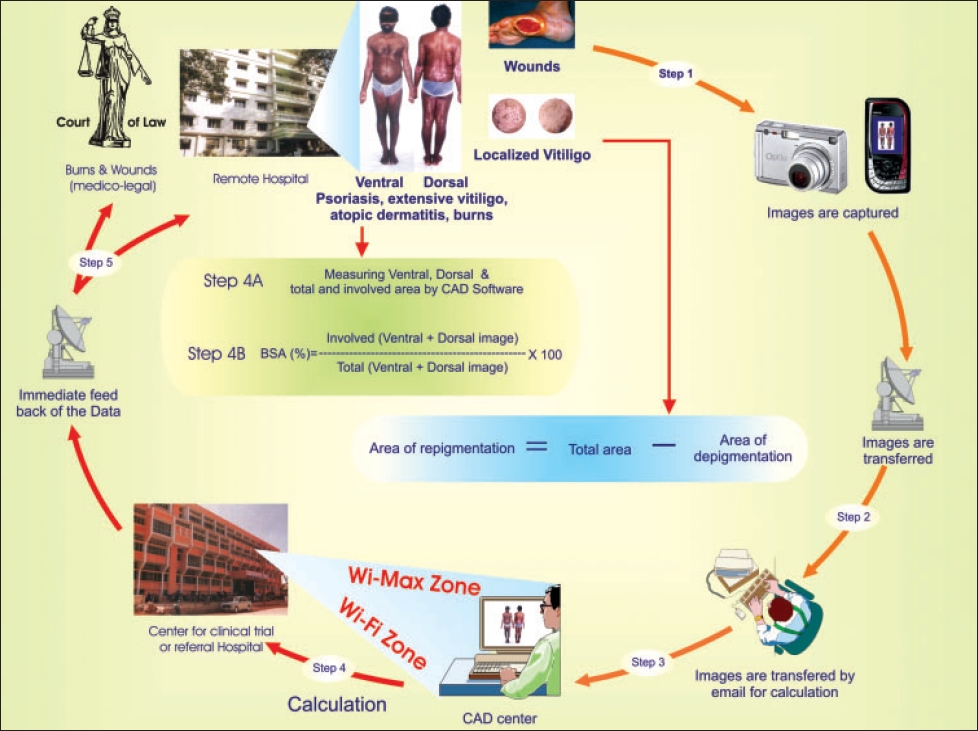 |
| The integration model to capture, transfer, measure and follow up skin lesions (generalized and localized), to deliver SAF teledermatology care |
|
| The integration model to capture, transfer, measure and follow up skin lesions (generalized and localized), to deliver SAF teledermatology care |
Introduction
The World Health Organization defines telemedicine as practice of healthcare using interactive audio, visual and data communications. It includes transfer of medical data, consultation, diagnosis and treatment, education and health care delivery. Telemedicine reduces travel, waiting time, treatment costs, minimizes follow-up visits and delivers specialty healthcare services to remote geographic regions.
Telemedicine is divided into:
- Real time or videoconference and
- Store and forward (SAF) system.
Real time or videoconference teledermatology (VCTD)
The dermatologist analyzes the patient by direct interaction using audio-video signals similar to face-to-face consultation through the videoconferencing equipment in the presence of a general practitioner or nurse. Diagnostic accuracy of VCTD ranges from 54 to 80%[1] (compared to face-to-face consultation considered as gold standard). Videoconference teledermatology achieves high levels of physician and patient satisfaction compared to store-and-forward teledermatology (SAFT), as there is direct and two-way interaction.
Store and forward teledermatology (SAFT)
The SAF stores patient data (digital images, clinical and demographic information) sent by general practitioners (GPs) in an electronic medium for future access by consultants in referral centers to deliver quality healthcare in remote geographic regions. Simultaneous presence of the clinician is not required. SAFT compared to VCTD is cheap, convenient for the healthcare provider with a high level of accuracy, however, it lacks the immediacy of direct patient contact.
Complete SAFT care equivalent to that of face-to-face consultation is essential. Given this background, the article reviews developments in 1) capture, store and transfer of the images, 2) computer-aided measurements of generalized and localized lesions and 3) the integration model to meet the above two requirements in a centralized location. This process enables diagnosis, management, periodic assessment and complete follow-up care to achieve physician and patient satisfaction.
Electronic devices, transfer medium and software used to capture, transfer and measure the skin images respectively are classified as follows:
Capture : Digital camera, cellular phone and personal digital assistants.
Transfer: Internet, Wi-Fi, Wi-Max and satellite communication (satcom based telemedicine network).
Measure: Computer-aided design (CAD) software
Developments in capture, store and transfer of skin lesions have been taking place by leaps and bounds.
Capture
Skin imaging for SAFT care has shown rapid progress. The availability of cost-effective photographic equipment and quick electronic transfer of high quality digital images favors SAFT. Digital cameras, cellular phones and personal digital assistants (PDA) promote capture, store and transfer.
Digital camera
SAFT uses digital camera with an average 640 x 480 pixels image resolution; a diagnosis agreement of 68%,[2] 89%,[3] 58%[4] and 48%[5] has been documented. The images are rapidly transferred[1] and stored in JPEG (Joint photographers expert group; http://www.jpeg.org) format using the internet. Diagnostic agreement varies from 41 to 95%.[6] It is low (48%)[5] for cutaneous malignancies. Poor image quality, lack of referral proforma data and cutaneous malignancies that are often difficult to diagnose with face-to-face contribute to poor agreement. SAFT promotes follow-up care in wound management by periodic monitoring of slough (concordance 84.6%), necrosis (concordance 98.2%) and granulation tissue formation (concordance 76.4%).[7]
Cellular phones
Inbuilt digital camera and networking features enable capture and transfer. Cellular phones[8] and Personal digital assistants[9] allow taking good quality images and sending them to the expert from remote geographic regions via a wireless network e.g., global system for mobiles (GSM) and universal mobile telecommunication system (UMTS). New generation cellular phones allow to take good quality images and transmit them directly to other cellular phones (via multi media messages) and computers (via e-mail or bluetooth wireless connection).[8] Cellular phones have a high potential to improve patient care as immediate image access and direct interaction are performed . A feasibility study[8] confirmed the importance of cellular phone in telemedical wound care. In 5% cases insufficient quality of images (after e-mail transfer) are noticed.[8] Transfer of skin images using cellular phones with a diagnosis agreement of 70% is documented.[10]
PDA
Laptops, handheld computers that are convenient to handle and offer combined features like camera, computing and networking are called PDA.[9] Massone et al[9] demonstrated the importance of PDA in teledermatology with a 79% diagnosis agreement.
Transfer (forwarding data)
The various media of data transmission are Internet, Wi-Fi, Wi-Max and Satellite communication (satcom-based telemedicine network), Digital lines called ′Integrated services digital network′ (ISDN) have data-carrying capacity or bandwidth from 128 kbps to 256 or 384 kbps.[1] Wi-fi and Wi-Max are super speed wireless network connections that enable high-speed transmission of the data. Wi-Fi is wireless fidelity that enables connections to mobile devices, digital camera, computers and personal digital assistants. Wi-fi uses radio waves and needs radio transmitter called router and receivers called access points (hotspots).The speed is 6Mbps. Superior to Wi-Fi is Wi-Max (worldwide interoperability for microwave access). It is a broadband wireless access technology providing super speed access at 70 mbit/s. Speed of the transfer medium is important for rapid and easy retrieval of large data. Therefore, a telemedical center should have Wi-Fi or Wi-Max installation for quality and speed of data transmission.
Satellite communication (Satcom-based telemedicine network)
Satellite connectivity is the feasible solution being demonstrated currently by the Indian space research organization (ISRO).[11] Cost-effective and rapid connectivity are achieved with satellite communication to reach inaccessible geographic regions where connectivity cannot be established through ISDN. Very small aperture terminals (VSAT) are used for this purpose. The complex network management is performed with a wide antennae installation called hub.
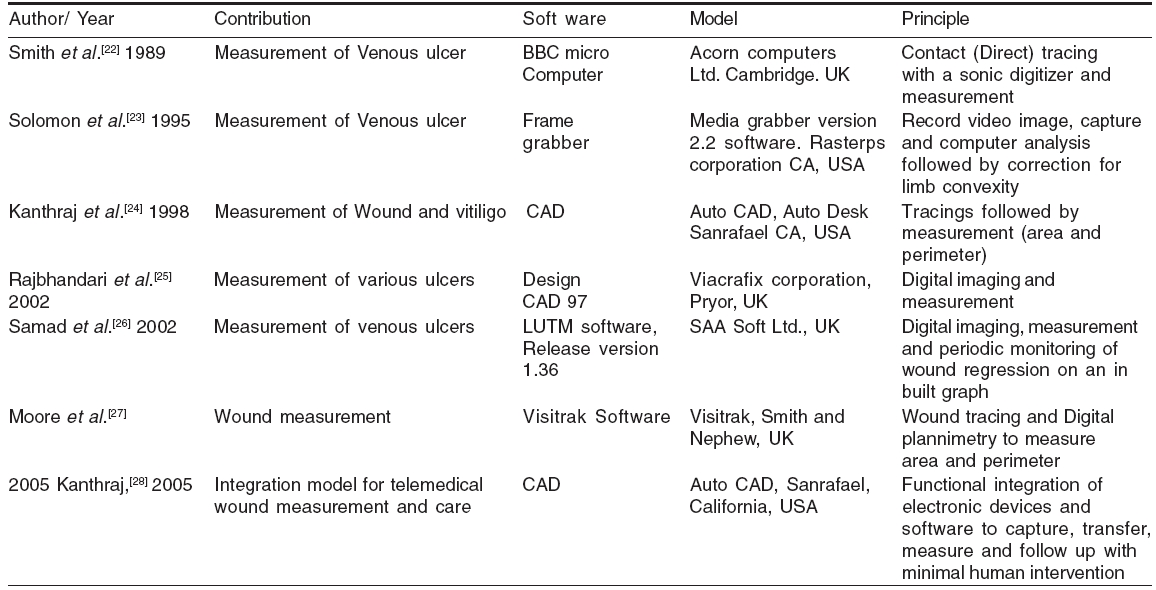
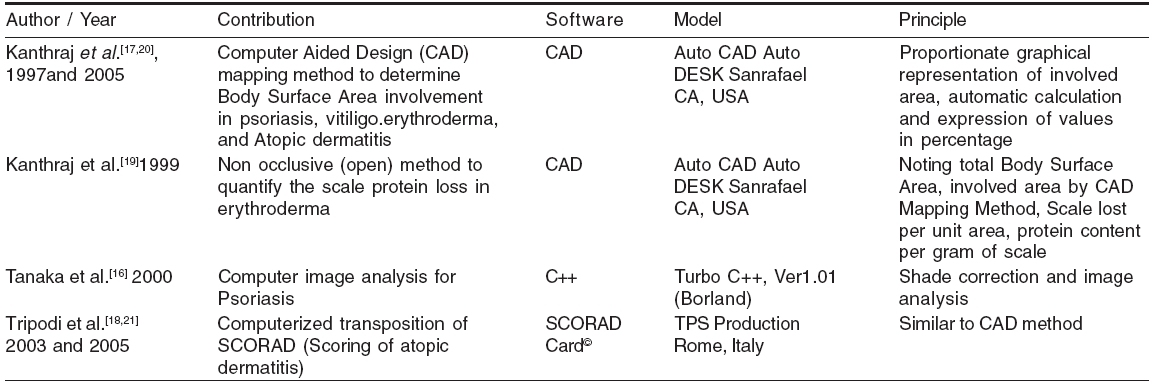
Developments in computer-assisted measurements of generalized and localized lesionsAssessment of melanoma by topodermatographic image analysis[12] and digital imaging of cutaneous lesions[13] are the early reports of measurements in digital imaging. Computer-aided image analysis to assess the extent of psoriasis,[14] computer-assisted planimetry from color photographs[15] and computer color segmentation methods[16] were developed. They[14],[15],[16] involve time-consuming processing of photographs and are technically demanding. To overcome these disadvantages CAD mapping[17] and SCORAD card[18] (Scoring of atopic dermatitis) are proposed. They are rapid and practical. Computerized wound measurements are calculated after digital imaging. [ Table 1],[Table - 2] summarize the developments[17],[18],[19],[20],[21],[22],[23],[24],[25],[26],[27] in computer-assisted measurements of generalized and localized lesions respectively.
The integration model for quality healthcare in remote areas[28]
Healthcare professionals in rural areas are the ′eyes′ for the expert. Computerized measurements are rapid, easy, precise and well suited for SAFT.
Inter and intraobserver variations in computerized measurements occur during capture of images. Mapping or tracing error could occur due to human intervention. To overcome these shortcomings the integration model is proposed.[28] This involves the systematic functional integration of electronic devices and software to capture, transfer, store, measure and follow up with minimal human intervention to deliver complete teledermatology care. Broadly it can be applied for a) generalized and b) localized lesions. The concept of the integration model is illustrated in [Figure - 1].
Setting up a teledermatology center[11]
Video-conference teledermatology
The hardware consists of a) computer b) video conferencing equipment c) and communication hardware.
Computer: It consists of desktop PC or Laptop (patient end), Desktop/Rack mount server at the telemedicine specialist counter (specialist end). Personal digital assistants or palmtops can also be used. Ideal computer- Pentium IV or above models with 512 MB of RAM having large hard disc (>10 GB) and 19" high-resolution monitor.
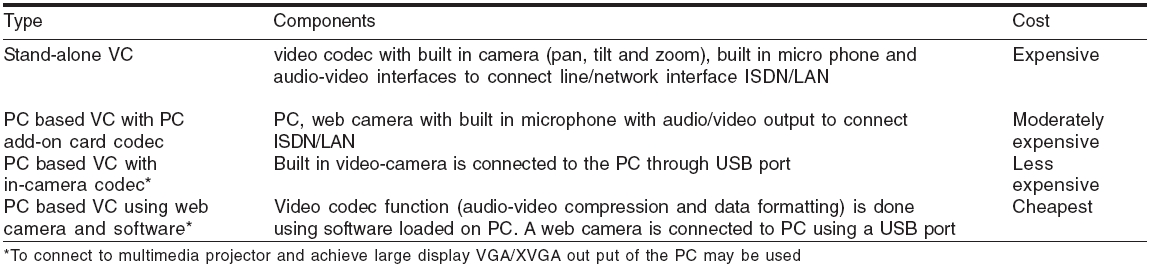
Videoconferencing equipment : Details are summarized in [Table - 3].
Communication hardware
i) Terrestrial: LAN (local area network), WAN (wide area network), ISDN, Internet.
ii) Wireless satellite: VSAT, wireless LAN, CDMA, GSM, GPRS.
We recommend readers interested in setting up a teledermatology center to go through the telemedicine manual.[11] The specific guidelines and recommendations for practice of telemedicine are recommended by the Indian Space Research Organization (ISRO) (www.isro.gov.in).
Mobile telemedicine unit
To benefit the grassroots population of rural India, ISRO and the ministry of information technology, Government of India have taken initiative towards health and education.[11] They have developed a mobile telemedicine unit. It operates using the satellite communication technology. It consists of telemedicine hardware, software and VSAT system mounted on a bus or a van. It can establish mobile telemedicine in any place.
The organization, functioning and beneficiaries of SAFT center[20],[29]
They are illustrated in [Figure - 2]. Incorporating CAD into the existing hardware of the institute avoids additional investment. Second, the existing computer programmer has basic CAD knowledge and there is no additional requirement of a new CAD programmer. The role of healthcare professionals is to capture and send the images and the programmer does the calculation and provides the results to dermatologists in the telemedical center. Business process organization (BPO) or computer professionals process without additional burden to the clinician. Therefore healthcare professionals at the telemedical center need not undergo training.
There is a delay to review the SAF consultation.[6] A referral hospital can have a fixed time on a day. The consultant can study the case with measurement as illustrated in the integration model [Figure - 1] before commencement of a teledermatalogy clinic. Relevant discussions are made, as both ends are prepared. Patient, general practitioners or nurse available in the given period, can interact by e-chat or webcam or voicemail for any clarifications required from the consultant. Whited et al .,[6] from the economic perspective of the United States Department of veteran affairs, observed SAFT to be costly. However, Zelickson et al .[30] noted SAFT to be cost-effective in nursing home settings. The process illustrated in [Figure - 2] and the multi-disciplinary approach makes CAD, SCORAD and SAFT accessible and economical for the healthcare providers.[20],[21],[31] They utilize these in a centralized location maximizing their utility and generalizability.
Imaging and the law
Photographs form important medico-legal evidence and play a vital role in the maintenance of dermatology records.[32] It has its special significance as digital images are used to capture, store, measure, transfer and deliver follow-up care. The image measurement is important for medico-legal evidence.
The US federal courts have ruled that digital images can furnish sufficient medical data to provide dermatological care.[32] The JPEG images [Table - 4] are generally sufficient rather than tag image file format (TIFF), hence storage in JPEG can be produced in the court of law.[32] Preservation of privacy and confidentiality of digital images in the era of teledermatology is important.[1],[33] Uniform rules, regulations and guidelines to capture, transfer, store and measure have to be framed in the interest of the patient, physician and government.
It may be possible that the referral center doctor is liable to be sued for mistakes made in diagnosis and management based on data and images alone. The legal principles of face-to-face consultation apply to any form of consultation.[1] A dermatologist must be conscious of the limitations of the equipment. In such cases when diagnosis is not sure they may offer differential diagnosis or no diagnosis and request for face-to face consultation and investigations to confirm the diagnosis.
Future directions
The mobile units utilize the V-SAT system developed by ISRO and are useful in HIV care, counseling, education and handling difficult dermatology cases in rural India. Under the GRAMSAT (Satellite communication-based technology for rural India) program ISRO has initiated several telemedicine pilot projects in 2001 specific to the needs of rural India.[11] It covers remote corners of Jammu, Kashmir, Ladakh, Andaman, Lakshadweep, northeastern regions and tribal districts like Chamarajnagar in Karnataka. A study revealed 81% cost saving in the Chamarajnagar district hospital, Karnataka using the SATCOM-based technology.[11] There is drastic reduction in travel cost that otherwise patients would have to incur while traveling to the neighboring districts. Such projects are useful in meeting the healthcare needs of remote and rural India. We have to join hands with the government and ISRO to answer the dermatology problems at the grassroots level of rural India.
On the other hand utilizing the integration model we should focus on computerized transposition of psoriasis, atopic dermatitis and vitiligo scoring system for periodic severity assessment and to deliver quality healthcare. The significant advantage in SAF is its ability to facilitate blinding in comparative studies. Wound care experts monitor as well conduct clinical trials in remote geographic regions.
Research in teledermatology is progressing in an arithmetic ratio (in additions) while advancement in information technology is progressing in geometric ratio (in multiples). High et al .[2] have cautioned that rapid technological advancement can render the existing technology obsolete before completion of traditional large-scale studies. We have to accelerate teledermatology research to deliver quality healthcare to remote geographic regions.
| 1. |
Eedy DJ, Wootton R. Teledermatology: A review. Br J dermatol 2001;144:696-707.
[Google Scholar]
|
| 2. |
Whited JD, Hall RP, Simel DL, Fog ME, Stechuchak KM, Drugge RJ, et al . Reliability and accuracy of dermatologists' clinic - based and digital image consultations. J Am Acad Dermatol 1999;41:693-702.
[Google Scholar]
|
| 3. |
High WA, Houston MS, Calobrisi SD, Drage LA, Mc Evoy MT. Assessment of the accuracy of low-cost store and forward teledermatology consultation. J Am Acad Dermatol 2000;42: 776-83.
[Google Scholar]
|
| 4. |
Tucker WF, Lewis FM. Digital imaging: A diagnostic screening tool? Int J Dermatol 2005;44:479-81.
[Google Scholar]
|
| 5. |
Mahendran R, Goodfield MJ, Sheehan-Dare RA. An evaluation of the role of a store -and -forward teledermatology system in skin cancer diagnosis and management. Clin Exp Dermatol 2005;30:209-14.
[Google Scholar]
|
| 6. |
Whited JD. Teledermatology research review. Int J dermatol 2006;45:220-9.
[Google Scholar]
|
| 7. |
Salmhofer W, Hofmann-wellenhof R, Gabler G, Rieger-Engelbogen K, Gunegger D, Binder B, et al . Wound teleconsultation in patients with chronic leg ulcers. Dermatology 2005;210:211-7.
[Google Scholar]
|
| 8. |
Braun RP, Vecchietti JL, Thomas L, Prins C, French LE, Gewirtzman AJ, et al . Telemedical wound care using a new generation of mobile telephones: A feasibility study. Arch Dermatol 2005;141:254-8.
[Google Scholar]
|
| 9. |
Massone C, Lozzi GP, Wurm E, Hoffman-Wellenhof R, Schoellnast R, Zalauder I, et al . Personal digital assistants in teledermatology. Br J Dermatol 2006;154:801-2.
[Google Scholar]
|
| 10. |
Massone C, Lozzi GP, Wurm E, Hoffman-wellenhof R, Schoellnast R, Zalauder I, et al . Cellular phones in clinical teledermatology. Arch Dermatol 2005;141:1319-20.
[Google Scholar]
|
| 11. |
Sathyamurthy LS, Bhaskaranarayana A. Telemedicine: Indian Space agency's (ISRO) initiatives for specialty health care delivery to remote and rural population. In : Sathyamurthy LS, Muthy RL, editors. Telemedicine manual-Guide book for practice of telemedicine, 1st ed. Indian Space Research Organization, Department of space. Government of India: Bangalore; 2005. p. 9-13.
In : Sathyamurthy LS, Muthy RL, editors. Telemedicine manual-Guide book for practice of telemedicine, 1st ed. Indian Space Research Organization, Department of space. Government of India: Bangalore; 2005. p. 9-13.'>[Google Scholar]
|
| 12. |
Voigt H, Classen R. Topodermatographic image analysis for melanoma screening and the quantitative assessment of tumor dimension parameters of the skin. Cancer 1995;75:981-8.
[Google Scholar]
|
| 13. |
Perednia DA, White RG, Schowengerdt RA. Localization of cutaneaous lesions in digital images. Comput Biomed Res 1989;22:374-92.
[Google Scholar]
|
| 14. |
Ramsay B, Lawrence CM. Measurement of involved area in patients with Psoriasis. Br J Dermatol 1991;124:565-70.
[Google Scholar]
|
| 15. |
Marks R, Barton SP, Shuttleworth D, Finlay AY. Assessment of disease progress in psoriasis. Arch Dermatol 1989;125:235-40.
[Google Scholar]
|
| 16. |
Tanaka M, Gaskell S, Edwards C, Marks R. Simple horizontal averaging programme enables shade correction for image analysis in psoriasis. Clin Exp Dermatol 2000;25:323-6.
[Google Scholar]
|
| 17. |
Kanthraj GR, Srinivas CR, Shenoi SD, Deshmukh RP, Suresh B. Comparison of computer aided design (CAD) and rule of nines methods in the evaluation of the extent of body involvement by cutaneaous lesions. Arch Dermatol 1997;133:922-3.
[Google Scholar]
|
| 18. |
Tripodi S, Panetta V, Pelosi S, Pelosi U, Boner AL. Measurement of body surface area in atopic dermatitis using specific PC software (SCORAD CARD). Pediatr Allergy Immunol 2004;15: 89-92.
[Google Scholar]
|
| 19. |
Kanthraj GR, Srinivas CR, Uma Devi P, Ganasoundari A, Shenoi SD, Deshmukh RP, et al . Quantitative estimation and recommendations for supplementation of protein lost through scaling in exfoliative dermatitis. Int J Dermatol 1999;38:91-5.
[Google Scholar]
|
| 20. |
Kanthraj GR. Computer aided design mapping for SCORAD index in atopic dermatitis - accessible and economical. Pediatr Allergy Immunol 2005;16:182-3.
[Google Scholar]
|
| 21. |
Tripodi S. Computer aided design mapping for SCORAD index in atopic dermatitis: SCORAD Card software. Pediatr Allergy immunol 2005;16;619.
[Google Scholar]
|
| 22. |
Coleridge Smith PD, Scurr JH. Direct method of measuring venous ulcers. Br J Surg 1989;76:689.
[Google Scholar]
|
| 23. |
Solomon C, Munro AR, Van Rij AM, Christie R. The use of video image analysis for the measurement of venous ulcers. Br J Dermatol 1995;133:565-70.
[Google Scholar]
|
| 24. |
Kanthraj GR, Srinivas CR, Shenoi SD, Suresh B, Ravikumar BC, Deshmukh RP. Wound measurement by computer aided design (CAD): A practical approach for software utility. Int J Dermatol 1998;37:714-5.
[Google Scholar]
|
| 25. |
Rajbhandari SM, Harris ND, Sutton M, Lockett C, Eaton S, Gadour M, et al . Digital imaging: An accurate and easy method of measuring foot ulcers. Diabet Med 1999;16:339-42.
[Google Scholar]
|
| 26. |
Samad A, Hayes S, French L, Dodds S. Digital imaging versus conventional contact tracing for the objective measurement of venous leg ulcers. J Wound Care 2002;11:137-40.
[Google Scholar]
|
| 27. |
Moore K. Using wound area measurement to predict and monitor response to treatment of chronic wounds. J Wound Care 2005;14:229-32.
[Google Scholar]
|
| 28. |
Kanthraj GR. The integration of the internet, mobile phones, digital photography and computer aided design software to achieve tele medical wound measurement and care. Arch Dermatol 2005;141:1470-1.
[Google Scholar]
|
| 29. |
Kanthraj GR. Computers or simple wound measurements: When Greek meets Greek, then comes the tug-of-war! Arch Dermatol 1999;135:992-4.
[Google Scholar]
|
| 30. |
Zelickson BD, Homan L. Teledermatology in the nursing home. Arch Dermatol 1997;133:171-4.
[Google Scholar]
|
| 31. |
Mallet RB. Teledermatology in practice. Clin Exp Dermatol 2003;28:356-9.
[Google Scholar]
|
| 32. |
Scheinfeld N. Photographic images, digital imaging, dermatology and the law. Arch Dermatol 2004;140:473-6.
[Google Scholar]
|
| 33. |
Goldberg DJ. Digital photography, confidentiality and teledermatology. Arch Dermatol 2004;140:477-8.
[Google Scholar]
|
Fulltext Views
2,217
PDF downloads
1,851





![[Table - 2]](#tbl_ijdvl_2007_73_1_5_30643_2.jpg){kind=link}
![[Figure - 1]](#fig_ijdvl_2007_73_1_5_30643_3.jpg){kind=link}
![[Table - 3]](#tbl_ijdvl_2007_73_1_5_30643_4.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2007_73_1_5_30643_5.jpg){kind=link}
![[Table - 4]](#tbl_ijdvl_2007_73_1_5_30643_6.jpg){kind=link}