Translate this page into:
Diagnosis of delayed pressure urticaria
Correspondence Address:
K V Godse
Shree Skin Centre, 22, L-market, Sector 8, Nerul, Navi Mumbai 400 706, Maharashtra
India
| How to cite this article: Godse K V. Diagnosis of delayed pressure urticaria. Indian J Dermatol Venereol Leprol 2006;72:155-156 |
 |
|
Sir,
Delayed pressure urticaria (DPU) is a physical urticaria in which pressure is the physical stimulus that causes whealing. Pressure (defined as the force applied to a unit area of surface) induces reproducible whealing in DPU. Delayed cutaneous erythema and edema occur in association with marked subcutaneous swelling after the application of a sustained pressure stimulus to the skin. These signs occur as early as 30 min and typically 4 to 6 h later. Lesions may persist for up to 48 h. The response is dependent on the degree of pressure; duration of the stimulus; body site affected; and activity of the disease, which is variable in intensity.[1] Sites that previously have reacted to pressure have been found to be refractory to an additional pressure stimulus for at least 24 to 48 h. Most patients with DPU have chronic idiopathic urticaria (CIU) and angioedema. DPU should be considered in all patients with CIU whose disease is unresponsive to antihistamines. The disease is variable and remissions and exacerbations occur.
In DPU, a positive response after any form of pressure challenge consists of the appearance of palpable lesions after at least 30 min. Because most positive responses occur at 6 h, observers usually read pressure tests at 6 h. There is no standard method of pressure testing for DPU. Hence, I used simple and easily available implements like a 2 kg weight and a blood pressure cuff to test for DPU in 50 patients of CIU.
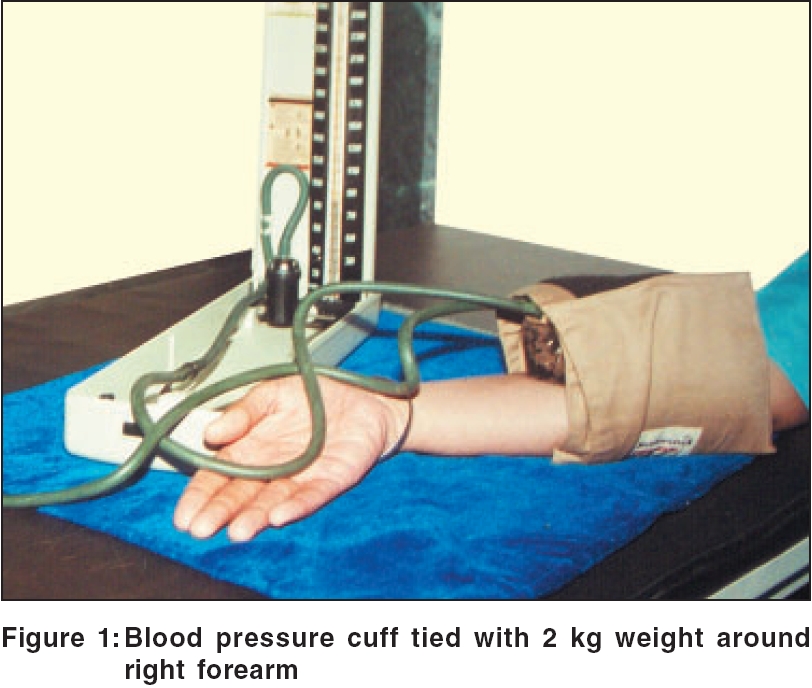
Fifty adult patients with chronic urticaria attending a private skin centre at Navi Mumbai were enrolled in this study. All antihistamines and oral steroids were stopped 48 h prior to the test. A 2 kg of weight, available at a general store, was placed on the right forearm of patients and a blood pressure cuff was strapped tightly around the weight to give sustained pressure [Figure - 1]. The pressure in the cuff is raised to 100 mm of Hg and is maintained for 1 min or till patient feels discomfort, whichever is earlier. Reading is taken after 30 min and at 6 h for visible and palpable swelling.
The 50 cases comprised of 33 male and 17 female patients (age range 18-80 years, mean age 43 years). Three patients (2 male and 1 female), out of the 50, tested positive with this instrument at 30 min and at 6 h. Positive test was seen as a palpable and visible swelling on right forearm at the site of pressure at the end of 30 min and at 6 h. These patients had typical history of swelling at the site of pressure, like waist and palms and soles.
In this test, we have tried to keep variables constant by using a standard 2 kg weight and a uniform pressure of 100 mm of Hg with the help of sphygmomanometer. Both the items can be easily procured. Patients should not be on antihistaminics or steroids for 48 h to prevent false negative test. In India, dermographometer is not available.
Ryan et al. tested for DPU by hanging a 15 lb weight at the end of a crepe bandage over the shoulder, thigh, or forearms of patients for at least 15 min.[2] Using this method, the area to which the force is applied is not defined; therefore, its reproducibility is not accurate enough for clinical trials, but the method is useful in clinical settings. Illig and Kunick designed an apparatus in which metal rods are held vertically in place, resting on a patient′s back, using a thick plastic sheet of material (PerspexÒ) to keep the rods in place. Adding more weights to the rods raised the pressure applied. The times of application of the pressure varied depending on the severity of the disease.[3] Modifications of this instrument have been used by other investigators studying DPU. Lawlor used a similar instrument with rods of 1.5 cm diameter and pressures of between 2.29 kg and 4.79 kg that were rested on the back for between 12 and 15 min.[4] Estes and Yung used a calibrated dermographometer to reproduce lesions in two patients. They applied pressures of 48, 73, 103, 136, 200 and 234 g/mm 2 for 10 s to the abdomen, arms and back and inspected the sites for up to 24 h. They showed a threshold whealing response of 136 g/mm 2 on the abdomen. By applying these pressures to the back for 5, 30, 60, 120 and 180 s respectively, they demonstrated that the time needed to produce a whealing response was inversely proportional to the degree of pressure applied.[5]
DPU is diagnosed infrequently, probably due to lack of interest in physical urticarias, unfamiliarity with the methods used to study the disease and the fact that chronic urticairia itself is frequently more severe in pressure-prone areas of the body (i.e., under belts or clothing). It is debatable as to whether this condition is mild DPU or is a pressure-induced worsening of chronic urticaria and angioedema.[1]
Summarizing, DPU is not uncommon in patients with chronic urticaria and this simple test is a valuable aid in a dermatologist′s office practice.
| 1. |
Lawlor F, Black AK. Delayed pressure urticaria. Immunol Aller Clin North Am 2004;24:247-58.
[Google Scholar]
|
| 2. |
Ryan TJ, Shim-Young N, Turk JL. Delayed pressure urticaria. Br J Dermatol 1968;50:485.
[Google Scholar]
|
| 3. |
Illig L, Kunick J. Klinick and diagnostik der physikalischen urticaria. Der Hautarzt 1969;20:167. [PUBMED abstract]
[Google Scholar]
|
| 4. |
Lawlor F, Barr R, Kobza BA, Cromwell O, Issacs J, Greaves M. Arachidonic acid transformation is not stimulated in delayed pressure urticaria. Br J Dermatol 1989;121:317.
[Google Scholar]
|
| 5. |
Estes SA, Yung CW. Delayed pressure urticaria: An investigation of some parameters of lesions induction. J Am Acad Dermatol 1981;5:25.
[Google Scholar]
|
Fulltext Views
1,886
PDF downloads
1,686





![[Figure - 1]](#fig_ijdvl_2006_72_2_155_25649_1.jpg){kind=link}