Translate this page into:
Changing trends in hair restoration surgery
Correspondence Address:
Mysore Venkataram
3437, 1st G Cross, 7th Main, Subbanna Garden, Vijayanagar, Bangalore - 560 040, Karnataka
India
| How to cite this article: Venkataram M. Changing trends in hair restoration surgery. Indian J Dermatol Venereol Leprol 2006;72:103-111 |
Abstract
Androgenetic alopecia is an important and common cause for baldness. Despite recent advances, the drug therapy of this condition remains unsatisfactory. Surgical hair restoration is the only permanent method of treating this condition. Introduction of recent techniques such as follicular unit transplantation have improved the cosmetic results and patient satisfaction. This article discusses the latest trends in hair restoration surgery. |
|
 |
|
 |
|
 |
|
Great things are done by a series of small things brought together.
- Vincent von Gough
Hair serves an important cosmetic function in humans and either the lack or excess of hair causes significant emotional stress. Pattern hair loss (androgenetic alopecia, PHL) represents the most common cause for baldness in men. The past decade has seen significant developments in the management of androgenetic hair loss. While medical therapy with both minoxidil and finasteride has a definite place in the management of male pattern hair loss (MPHL), its effect is temporary and the results are not satisfactory in advanced pattern hair loss. Surgical management remains the only permanent method of restoring hair in PHL. This article reviews the recent trends in the surgical management of male PHL.
Etiology of pattern baldness[1],[2]
The term androgenetic alopecia (pattern baldness) has evolved from its dependence on the twin factors of androgens and genetic background. Pattern hair loss is probably multifactorial and may be inherited as an autosomal dominant trait with variable penetrance. The responsible genes have not yet been identified.
Although the term is used for both males and females, there are considerable differences between the sexes. Male pattern alopecia often presents in the first decade after puberty and is characterized by deep bitemporal recession and balding of the vertex, whereas female pattern alopecia, which commonly presents in 4th to 5th decades, is more diffuse, without bitemporal recession.
It is doubtful whether the hair loss seen in women is primarily androgen dependent and it is possible that several other factors may be responsible; hence the term ′female pattern hair loss (FPHL)′ is preferred to the term androgenetic alopecia when referring to women with this type of alopecia.[2],[3] One noteworthy feature in both female and male pattern hair loss is that occipital scalp is spared of this process and the hairs in this region persist for life.
Mechanism of pattern baldness[1],[2]
Follicular miniaturization is the main event that characterizes pattern hair loss. In androgenetic alopecia, follicles undergo miniaturization, shrinking from terminal to vellus-like hairs, about 1 cm in length. The anagen duration decreases, more balding follicles are projected into telogen and hair shedding increases. In miniaturization, the duration of anagen may shrink from the normal of 3-5 years to 1 month, but the duration of telogen (3 months) remains the same. This is accompanied by a prolongation of the lag phase or kenogen, after telogen.
The reason why the occipital hair is spared of this process is not entirely clear. For reasons that are not known fully, occipital scalp is not androgen dependent. One hypothesis is that the dermis in the occipital area is derived from cephalic mesoderm, whereas the dermis over the rest of the scalp comes from neural crest derivatives. Whatever the reason, the fact that occipital hairs are permanent serves as the basis of hair transplantation.[4]
Treatment of pattern baldness
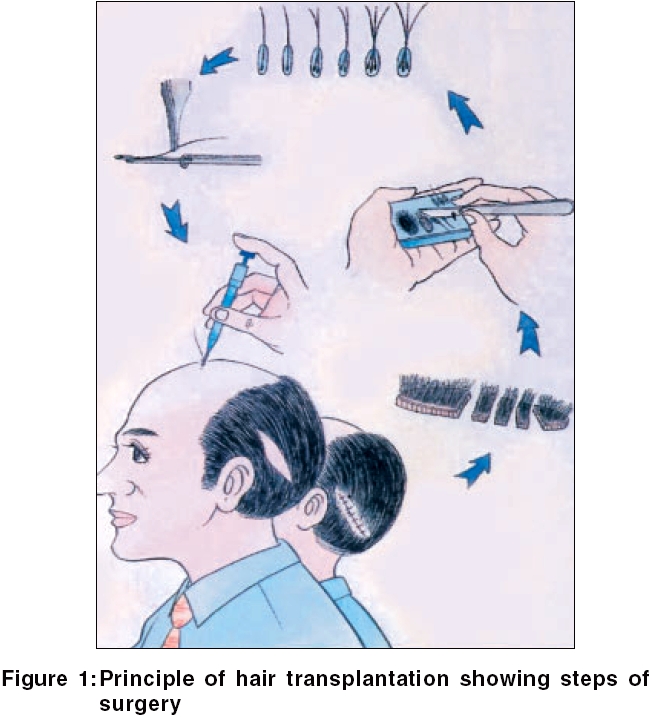
While drugs such as minoxidil, finasteride and duasteride represent significant advances in the management of MPHL, the fact that their action is temporary and the hairs are lost after stopping therapy continues to be a major limitation.[5],[6] In view of this, surgical hair restoration remains the only permanent method of treating pattern baldness. The basis of hair transplantation, as explained above, is that occipital hairs are never lost and, more importantly, they show donor dominance and hence can be transplanted in the balding area [Figure - 1].[4]
History and evolution of hair transplantation[7]
It is important to understand how the technique has evolved over the decades. In 1959, Norman Orentreich first established the concept of ′donor dominance′ in MPHL and successfully used 6-12 mm punches to create grafts in the occipital area.[4] These grafts were then transplanted to the bald area and hairs grew successfully. This method, though an easy procedure, had two major disadvantages: The large punches resulted in a highly unnatural ′doll look′ or ′paddy field look′ over the recipient area; and in addition, the donor site on occipital area was full of punched out scars, thus making future transplants more difficult. In hindsight, it seems paradoxical that in a paper published in a Japanese journal in 1944, a Japanese surgeon, Hajime Tamura, had demonstrated that ′the smaller the graft, better the results.′[8] However, this valuable advice was lost to the world because of World War II and what was taught by Orentreich became the accepted method for nearly three decades, with unsatisfactory results for a generation of patients, bringing disrepute to the technique. By the late 1970s, the Japanese advice was rediscovered and the era of minigrafts and micrografts started.[9],[10] Also, instead of the use of a punch to create grafts from the donor area, single-strip dissection was adopted.[9] This had the advantage of avoiding multiple scars and preserved the occipital area for future grafts. Another advance in donor strip dissection was the introduction of the multibladed knife (which included 3-4 blades) to cut out multiple 2 mm wide strips in the donor area, resulting in faster dissection and lesser dissection time.[11],[12] However, the use of the multibladed knife has now been given up as it results in significant transection of hairs. The donor strip was dissected by vertical sectioning with a blade to create minigrafts (5-6 hairs) and micrografts (3-4 hairs). This method, called minimicrografting, became popular in the 80s and early 90s. Though punches of sizes 1.5-3 mm were still used in the recipient area, round holes had the disadvantages of causing either pitting or cobble stoning and hence other instruments such as linear slits, 15 number blade, NoKor needles and 16/18 gauge needles came to be used for creating recipient sites.[13],[14] A transplant session in the early 80s would transplant about 600-800 grafts, with 1-2 assistants and last 2-3 hours. Each patient needed 2-3 surgeries for proper results.
Concept of follicular unit[15],[16]
In 1984, Headington published his now classic paper in which it was demonstrated by transverse sections of scalp biopsies, that hairs did not occur singly, but as naturally occurring groups that were referred to as the follicular unit (also referred to as bundles).[15] Each unit consisted of 1 to 4 terminal follicles; 1, or rarely 2, vellus follicles; associated sebaceous lobules and insertions of the arrectores pili; perifollicular vascular plexus and neural net; and perifollicular collagen. This paved the way, in 1990s, for the ′Rolls Royce of hair transplantation′ follicular unit transplantation (FUT), which has now become the gold standard for hair transplantation.[17] Follicular unit transplantation is a method of hair restoration surgery by which hair is transplanted exclusively in its naturally occurring individual follicular units.
Logic of follicular unit transplantation[18],[19],[20],[21]
Follicular unit transplantation has several important features:
· Whether they contain 1, 2, 3, or 4 hairs, the grafts (units) are nearly of the same size and hence, one need to create small sites of roughly the same size to transplant them
· Smaller sites help in denser packing of grafts
· With smaller sites, the bleeding is less
· The look is more natural
Thus, it is a way to get the most hairs into the smallest possible site and create the smallest wound. This is referred to as a snug fit.
Mathematics of FUT[20],[22],[23]
Studies have demonstrated that the number of follicular units/cm 2 is nearly constant in all individuals, with normal density being 100 follicular units/cm 2 and the number of hairs per unit varies from 1 to 4 and rarely 5 per unit. Hence, the number of hairs/cm 2 varies from person to person. What determines the number of hairs in a person is the number of hairs per unit and not the number of units, which is nearly constant in all individuals. Since the follicular unit density is relatively constant; the same number of follicular units is needed to cover a specific size of bald area regardless of the hair density of the patient. Also, a person can lose half the number of his hairs before he appears bald.
Calculation of grafts[23]
A typical patient has 50,000 follicular units (100,000 hairs, assuming 2 hairs per unit) on his scalp. Of these, 75% (37,500) are on the frontal scalp and vertex and hence are at risk of being lost. The occipital (permanent donor) area has 25% of the total hairs on the scalp (25,000 hairs or 12,500 units). Since a person can afford to lose half his hairs before he appears bald, of the 12,500 donor units, approximately half are available for harvesting (i.e., 6250). If one assumes 100 units per sq cm, one can harvest roughly 1700 follicular unit grafts (consisting of about 3400 hairs) in a donor strip of 14 cm x 1.2 cm.
Calculation of the number of hair units required for the recipient area[22],[23]
0The frontal area is triangular and the area is calculated by the formula ½ x breadth x height. The vertex is circular and its area is calculated by the formula: A = pr 2 (A = area, p = 3.14, r = radius). For the reasons mentioned above, only half the total bald area has to receive the grafts to get good cosmetic results. If a person has frontal baldness of 30 cm 2, the normal density would be 3000 follicular units. By the above logic, the required number of units for a good cosmetic look in the same area would only be 1500 grafts. Therefore, it is obvious that one needs to perform large sessions exceeding 1000-1500 units in most cases to get a good cosmetic appearance. This has to lead to the so-called mega-sessions.
Why mega-sessions?[20],[24],[25],[26]
A session in which more than 1000 units are grafted is called a mega-session. It has several advantages:
· It avoids multiple surgeries and the resulting absence from work
· In multiple grafts, the first graft always yields the best results
· A large session economizes donor supply
For these reasons, small sessions, though technically easy, are discouraged and large sessions are performed in most centers worldwide.
Role of microscopic dissection[27],[28],[29]
Microscopic dissection using a dissecting microscope represents a major advance in hair restoration surgery and has become the standard practice in most advanced centers as it helps in better visibility and recognition of follicular units, more accurate dissection and minimizes transection of hairs. However, it also slows down the procedure and needs trained staff, resulting in an increased cost for the patient.
Micrografts/minigrafts vs follicular unit transplants[20],[30],[31],[32],[33]
The basic difference is that in micrografts, grafts are separated by random dissection and vertical strokes by a blade without consideration of the architecture of the follicular units, without the assistance of microscope. Hence, dissection of micrografts is faster, but vertical dissection may disrupt units. In addition, micrografts are thicker than follicular units and hence need larger holes for insertion. However, despite the superiority of FUT, it should be recognized that many surgeons continue to perform minigrafts and micrografts with satisfactory results.
Limitations of follicular unit transplantation[19]
FUT has several disadvantages:
· Follicular unit dissection is exacting and requires special skill
· Follicular units are delicate and require special handling
· Follicular unit transplantation is labor intensive and time consuming
· FUT needs microscopic dissection of hairs
· FUT needs more assistants and is more expensive
In view of these limitations, several authors have used follicular unit pairing or multiunit grafting (MUG).[32],[33] In this method, two or three closely packed units are dissected as one graft and are inserted into a single recipient site. Since the units contain 1, 2 or 3 hairs, a MUG may consist of 3, 4, 5 or 6 hairs. This method helps in reducing the time for both dissection and insertion. This method needs experience on the part of the dissector to choose such closely packed units. Also, such units should be inserted only in the center and hind areas and not in the hairline, to ensure a good cosmetic result.
Role of automation[20],[21],[34]
Hair transplantation has remained a manual process, a labor-oriented technique than an instrument-oriented one. Several efforts have been made to introduce instruments, thereby reducing the manual work and time. These include the rapid-fire carousel of Rassman, implanters of Chow and Kim, Calvitron and the Mangubatt dissector. However, these instruments have limitations and their use has been limited.
In the early 90s, the CO 2 laser and later the erbium YAG laser were introduced to make recipient sites. The advantages claimed are ′less bleeding′ and ′uniform holes.′ However, thermal coagulation of the recipient bed caused by a laser can lead to poor hair growth. Hence, the role of lasers in hair transplantation continues to be a debatable issue.
Density in hair transplantation[37],[38],[39]
As explained earlier, the normal hair density is around 100 units/cm 2.[16],[20] Obviously, because the donor area is only a third of the total balding area, it is not possible to achieve this density in any hair restoration surgery. Generally, the density achieved is between 30-40 units/cm 2. Reports of a higher density (called dense packing) of 55-60 units/cm 2 have been made, but graft survival and the final yield after such dense packing is a matter of debate.
Factors determining outcome in hair transplantation[18],[19],[25],[26],[40],[41]
· An important factor is the hair density, as previously explained
· Hair diameter is also an important factor in contributing to the appearance of fullness after surgery. Thick hair (90 microns in diameter) has three times the volume of thin hair (50 microns diameter)
· Color of hair: Black hair shines against bald scalp and hence is less suited than gray hair
· Curly hair can cover a larger area than straight hair
These inherent factors are thus very important. In India, the author′s experience is that patients from Kerala and Tamil Nadu have thick hair, a high hair density (2.7 hairs/ follicular unit) and are very suitable candidates for surgery.
Procedure of follicular unit hair transplantation
Patient selection: Who should undergo hair transplantation?[5],[41]
Proper patient selection is extremely important. Patients in their early twenties with early thinning of hair are not good candidates as the pattern of hair loss is yet to be established. Further, though highly motivated, these patients are often obsessed about their disability and have unrealistic expectations. Hence they need to be properly counseled and given medical therapy. Likewise, patients with advanced baldness may not have sufficient donor hair and hence may not represent good candidates. The ideal candidates are patients with established baldness in their late twenties, thirties or forties, without significant systemic health problems and with realistic expectations.
Informed consent should be obtained after detailed counseling session, which includes:
· Discussion on the different management options available
· Detailed explanation about the surgical procedure and possible postoperative complications
· Specific instructions that result would be seen only after 8-9 months
· In young patients the specific instruction that continued drug therapy is necessary to preserve the existing hair
· Patients should not expect to get the same amount of hair that they had before balding
· Patients should understand that hair transplantation is a cosmetic procedure and will not affect the underlying process of baldness, which may continue in future
· Any allergies or medical condition that the patient may have should be recorded
Preoperative procedures
These are routine and include:
· Advice to stop smoking as smoking increases intraoperative bleeding
· Avoidance of vigorous exercise
· Use of ketoconazole shampoo if the patient has dandruff
· To avoid oral NSAIDs as they may increase intraoperative bleeding
· A tranquillizer such as diazepam or lorazepam the night before surgery
Preparation of the patient
· Preoperative antibiotic such as ofloxacin and a preoperative tranquillizer such as diazepam or lorazepam.
· The donor site hairs are trimmed to a length of about 2-4 mm. The location of the strip is just above the occipital protuberance, extending from one ear to the other. Too low a strip will lead to poor healing while too high a strip will lead to the possibility of donor hair being in the androgen-dependent balding area. Likewise, temporal hairs are not included as the scar may be visible. The length of the strip depends on the number of grafts required. Generally, for a 1500 follicular unit session, a strip 15 cm long and 1.2 cm wide would be sufficient in a patient with a follicular unit density of 100 units
· Surgical cleaning of the donor area with povidone iodine
Lignocaine 2% with adrenaline is injected slowly using a 26 gauge needle both into the subcutis and the papillary dermis in the occipital area. Since the nerves in the occipital area run upwards, the lower border of the strip should be injected. In addition, about 50 ml of normal saline with 0.5 ml epinephrine is used to tumesce the donor strip. Tumescence has the advantage that it produces vasoconstriction and reduces intraoperative bleeding. It also lifts the subcutis from the underlying vessels and prevents damage to large vessels and nerves. Proper monitoring of the patient is important. A digital pulse oximeter is ideal for this purpose. The presence of an anesthetist or a nurse trained in emergency medical care and life support is desirable. The total amount of lignocaine should be carefully watched to avoid lignocaine toxicity. It is advisable not to exceed a total cumulative lignocaine dosage of 7 mg/kg body weight.
Donor dissection[Figure - 2][45],[46],[47]
A multibladed knife yields multiple strips and hence makes dissection easier, but it also results in transection of hairs up to 20% and hence should be avoided. A single strip of skin is excised by elliptical excision with a number 11 sized scalpel blade. The strip′s width should be about 1.2-1.5 cm. The angle of dissection should at all times be parallel to the direction of hair to avoid transection of hairs. It is important that the dissection is performed at the mid-subcutis level and should not go deeper in to the galea; the latter not only increases bleeding but also leads to poor postoperative healing with a wider scar. The author does not prefer undermining of edges as it may result in excessive bleeding. Vicryl or 3-0 silk is used to suture the strip by either continuous or intermittent sutures. Absorbable sutures such as monocryl (which gets absorbed in 2 weeks) can be used, particularly for outstation patients.[47] Tension should be avoided while suturing, to avoid a wide scar. Staples can be used instead of suture, but they may cause more postoperative pain. The suture site is dressed with a pad and fixed with a headband.
Dissection of hairs [Figure - 3][Figure - 4][27],[28],[29],[47],[48],[49],[50]
This is perhaps the most important step in the procedure. The elliptical strip is first dissected into small slivers of 1 or 2 follicular unit width (1-2 mm) under a stereomicroscope. This crucial step needs microscopic dissection to avoid transection of hairs. The slivers are then dissected into units of 1-4 hair units either under a magnifying loupe or a microscope [Figure - 3]. In the author′s experience, in Indian patients slivers can be safely dissected into units without significant transection under loupe magnification or even with the naked eye as the roots are pigmented [Figure - 4]. It is important to avoid damage to the hair root to avoid too much fat in the graft and to avoid vigorous handling of the grafts. Whether the grafts should be skinny (thin) or chubby (thick with a little amount of dermis around them) is a matter of debate.[51],[52] Skinny grafts need smaller recipient sites and can be packed densely, but very fine dissection has the risk of damaging the arrectores pili muscle, sebaceous glands and telogen hairs, which may be important in hair growth. Skinny grafts also need more careful handling to avoid damage. Grafts are very susceptible to drying and hence they should be kept in cold saline. The dissected hairs are grouped according to the type of units (1, 2, 3 or 4 hairs) separately on pieces of gauze or cloth in Petri dishes containing saline. It is also important for the dissectors to keep count of the number of grafts dissected. Dissection of hairs is a skilled job, needing adequate training. Proper lighting and seating arrangements for the dissecting team are important to ensure proper visualization and to avoid fatigue.
Recipient area anesthesia
The local anesthetic (2% lignocaine with adrenaline) is injected along the proposed hairline in a ring shaped pattern as the nerves run upwards from below. A supraorbital block and supratrochlear block may be additionally given to reduce the amount of lignocaine needed. After this ring anesthesia, tumescent saline solution is then injected in the entire donor area.
Recipient site-graft insertion[19],[21],[25],[26],[35],[52]
Punches are not generally preferred for creating recipient sites because of the following disadvantages:
· Punch wounds heal with either cobble stoning or pitting
· Punched out skin has to be removed each time and hence slows the procedure
· Round holes lead to loss of tissue and more bleeding
Hence, other instruments such as NoKor needles (size 16 for three-hair units, size 18 for two-hair units), slits (for combination grafts), rectangular punches, 18/19 size needles (for 1- to 2-hair units) and blades of different sizes are used.
There are several methods for insertion:
a) The ′stick and place method′ involves making a recipient site, followed immediately by insertion of hairs into the site by an assistant
b) Creating all the required recipient sites at one time and then placing the grafts one by one
Each method has its advocates. The direction of donor sites should be parallel to the direction of existing hairs. In patients with advanced baldness, where there are no existing hairs, the direction of miniature hairs should be noted. The hairs are generally at an angle of 45° to the scalp. Single-hair units are preferred for the hairline, while 2-, 3- or 4 - hair units are packed behind the hairline. The depth of the donor site should generally be 4-5 mm to avoid damage to deeper vessels. During insertion, it is important to avoid vigorous handling of grafts and to insert them in a smooth manner in the direction of the creation of the site. Generally, the insertion is done from back to front to avoid popping. The donor site should be cleaned frequently with saline to avoid clogging of blood.
Postoperative instructions
In follicular unit transplantation, a simple cap-like dressing is adequate, which too can be removed the very next day. This is because the ′snug fit′ ensures that postoperative bleeding is minimal. Analgesics such as tramadol are prescribed for pain. An antibiotic such as ofloxacin should be continued for 5 days. Shampooing is started the very next day to remove crusts.
Postoperative complications[54],[55]
The most common complication is postoperative pain, which needs to be managed by proper use of analgesics. Swelling over the forehead occurs in about 25% of patients on day 3 of surgery due to postoperative edema and the presence of large amount of saline injected during anesthesia. This is temporary and can be managed with ice compresses and administration of a short course of oral steroids. Infection is rare. Drug-induced gastritis, persistence of crust at the recipient sites, persistent pain at the donor site, sterile pustules during the second month (caused by an irritant reaction during hair growth) are some of the other common but minor complications. Keloid formation is rare. Delayed hair growth is another complication.[55]
Follow-up
Generally no follow-up is required. The grafted hairs may start falling at 2 weeks due to postoperative telogen effluvium. The hairs start growing by 3-4 months at the rate of one cm every month, with full cosmetic results at the ninth month. Minoxidil is started in the second week to promote hair growth and prevent delayed results.[5],[6]
Follicular unit transplantation has established itself as the standard method of hair transplantation. Mega-sessions, single-strip dissection and microscopic dissection have all added to the enhanced efficacy of the procedure and resulted in highly satisfactory results. It is now possible for trained hands to perform sessions of nearly 2000 grafts. The field of hair transplantation has long suffered from poor results caused by punch transplantation and has now got its due place in cosmetic surgery. It is also important to recognize that enthusiastic but novice surgeons without proper training are bringing disrepute to the technique. Hence, for satisfactory results, the surgery should be performed by a dermatosurgeon who is properly trained and has a team of well-trained assistants.
| 1. |
Whiting DA. Possible mechanisms of miniaturization during androgenetic alopecia or pattern hair loss. J Am Acad Dermatol 2001;45:S81-6.
[Google Scholar]
|
| 2. |
Alfredo Rebora. Pathogenesis of androgenetic alopecia. J Am Acad Dermatol 2004;50:777-9.
[Google Scholar]
|
| 3. |
Chartier MB, Hoss DM, Grant-Kels JM. Approach to the adult female patient with diffuse nonscarring alopecia. J Am Acad Dermatol 2002;47:6.
[Google Scholar]
|
| 4. |
Orentreich N. Autografts in alopecias and other selected dermatological conditions. Ann N Y Acad Sci 1959;83:463-79.
[Google Scholar]
|
| 5. |
Bouhanna P. Androgenetic alopecia: Combining medical and surgical treatments. Dermatol Surg 2002;28:136-42.
[Google Scholar]
|
| 6. |
Avram MR, Cole JP, Gandelman M, Haber R, Knudsen R, Leavitt MT, et al . The potential role of minoxidil in the hair transplantation setting. Dermatol Surg 2002;28:894-900.
[Google Scholar]
|
| 7. |
Unger WP. The history of hair transplantation. Dermatol Surg 2002;28:1035-42.
[Google Scholar]
|
| 8. |
Tamura H. Hair grafting procedure. Jap J of Dermatol Venereol [Japanese] 1943;2;52. [Quoted in Unger WP. The history of hair transplantation. Dermatol Surg 2002;28:1035-42.]
[Google Scholar]
|
| 9. |
Unger WP. Suturing of donor sites. In: Unger WP, editor. Hair transplantation. Marcel Dekker: New York; 1979. p. 64.
[Google Scholar]
|
| 10. |
Seager DJ. Micrograft size and subsequent survival. Dermatol Surg 1997;23:757-61.
[Google Scholar]
|
| 11. |
Brandy DA. A new instrument for expedient production of minigrafts. J Dermatol Surg Oncol 1992;18;468-72.
[Google Scholar]
|
| 12. |
Brandy DA. New instrumentation for hair restoration surgery. Dermatol Surg 1998;24:629-31.
[Google Scholar]
|
| 13. |
Brandy DA, Meshkin M. Utilization of No-Kor Vented needles for slit-micrografts. J Dermatol Surg Onc 1994;20:336-9.
[Google Scholar]
|
| 14. |
Arnold J. Mini-blades and a mini-blade handle for hair transplantation. Am J Cosm Surg 1997;14:195-200.
[Google Scholar]
|
| 15. |
Headington JT. Transverse microscopic anatomy of the human scalp. Arch Dermatol 1984;120:449-56.
[Google Scholar]
|
| 16. |
Jimenez F, Ruifernandez JM. Distribution of human hair in follicular units. A mathematical model for estimating the donor size in follicular unit transplantation. Dermatol Surg 1999;25:294-8.
[Google Scholar]
|
| 17. |
Bernstein RM, Rassman WR, Szaniawski W, Halperin A. Follicular transplantation. Int J Aesth Rest Surg 1995;3:119-32.
[Google Scholar]
|
| 18. |
Bernstein RM, Rassman WR. The aesthetics of follicular transplantation. Dermatol Surg 1997;23:785-99.
[Google Scholar]
|
| 19. |
Stough DM, Whitworth JM. Methodology of follicular unit hair transplantation. Dermatol Clin 1999;17:287-306.
[Google Scholar]
|
| 20. |
Bernstein RM, Rassman WR. The logic of follicular unit transplantation. Dermatol Clin 1999;17:277-95.
[Google Scholar]
|
| 21. |
Bernstein RM, Rassman WR. Follicular unit hair transplantation. Dermatol Surg 1997;23:771-84.
[Google Scholar]
|
| 22. |
Bernstein RM. Measurements in hair restoration. Hair Transplant Forum International 1998;8:27.
[Google Scholar]
|
| 23. |
Chang SC. Estimation of number of grafts and donor area. Hair Transplant Forum Int 2001;11:101-3.
[Google Scholar]
|
| 24. |
Rassman WR, Carson S. Micrografting in extensive quantities: The ideal hair restoration procedure. Dermatol Surg 1995;21:306-11.
[Google Scholar]
|
| 25. |
Uebel CO. The punctiform technique with the 1000-graft session. In: Stough DB, Haber RS, editors. Hair Transplantation: Surgical and medical. St. Louis; Mosby-Year Book Inc. 1996. p. 172-7.
[Google Scholar]
|
| 26. |
Limmer BL. Thoughts on the extensive micrografting technique in hair transplantation. Dermatol Surg 1996;6:8.
[Google Scholar]
|
| 27. |
Limmer BL. Elliptical donor stereoscopically assisted micrografting as an approach to further refinement in hair transplantation. Dermatol Surg 1994;20:789-93.
[Google Scholar]
|
| 28. |
Seager D. Binocular stereoscopic dissecting microscopes: Should we use them? Hair Transplant Forum Int 1996;6:2-5.
[Google Scholar]
|
| 29. |
Bernstein RM, Rassman WR. Dissecting microscope vs magnifying loops with transillumination in the preparation of follicular unit grafts: A bilateral controlled study. Dermatol Surg 1998;24:875-80.
[Google Scholar]
|
| 30. |
Bernstein RM, Rassman WR, Seager D, Shapiro R, Cooley JE, Norwood OT, et al. Standardizing the classification and description of follicular unit transplantation and mini-micrografting techniques. Dermatol Surg 1998;24:957-63.
[Google Scholar]
|
| 31. |
Brandy DA. A technique for hair-grafting in between existing follicles in patients with early pattern baldness. Dermatol Surg 2002;26:801-5.
[Google Scholar]
|
| 32. |
Brandy DA. The art of mixing follicular units and follicular groupings in hair restoration surgery. Dermatol Surg 2002;28:320-8.
[Google Scholar]
|
| 33. |
Unger W. Different grafts for different purposes. Dermatol Surg 1997;14:177-83.
[Google Scholar]
|
| 34. |
Choi YC, Kim JC. Single hair transplantation using the Choi hair transplanter. J Dermatol Surg Oncol 1992;18:945-8.
[Google Scholar]
|
| 35. |
Bernstein RM, Rassman WR. Laser hair transplantation: Is it really state of the art? Lasers Surg Med 1996;19:233-5.
[Google Scholar]
|
| 36. |
Fitzpatrick RE, Marchell NL. Laser hair transplantation II. Dermatol Surg 2000;26:181-9.
[Google Scholar]
|
| 37. |
Limmer B. The density issue in hair transplantation. Dermatol Surg 1997;23:747-50
[Google Scholar]
|
| 38. |
Unger WP. Density issue in hair transplantation. Dermatol Surg 1998;24:297.
[Google Scholar]
|
| 39. |
Marritt E. The death of the density debate. Dermatol Surg 1999;25:654-60.
[Google Scholar]
|
| 40. |
Rassman WR. Concern about quality. Hair Transplant Forum Int 1994;4:3.
[Google Scholar]
|
| 41. |
Bernstein RM, Rassman WR. Follicular transplantation: Patient evaluation and surgical planning. Dermatol Surg 1997;23:771-84.
[Google Scholar]
|
| 42. |
Nussbaum BP. Reducing pain during hair transplant lidocaine infiltration. Dermatol Surg 2001;27:98.
[Google Scholar]
|
| 43. |
Seager DJ, Simmons C. Local anesthesia in hair transplantation.Dermatol Surg 2002;28:320-8.
[Google Scholar]
|
| 44. |
Nusbaum BP. Techniques to reduce pain associated with hair transplantation: Optimizing anesthesia and analgesia. Am J Clin Dermatol 2004;5:9-15.
[Google Scholar]
|
| 45. |
Seery GE. Hair transplantation: Management of donor area.Dermatol Surg 2002;28:136-42.
[Google Scholar]
|
| 46. |
Brandy DA. Intricacies of the single-scar technique for donor harvesting in hair transplantation surgery. Dermatol Surg 2004;30:837-44.
[Google Scholar]
|
| 47. |
Bernstein RM, Rassman WR. A new suture for hair transplantation: Poliglecaprone 25. Dermatol Surg 2001;27:5-11.
[Google Scholar]
|
| 48. |
Cooley J, Vogel J. Loss of the dermal papilla during graft dissection and placement: Another cause of x-factor? Hair Transplant Forum Int 1997;7:20-1.
[Google Scholar]
|
| 49. |
Kurata S, Ezaki T, Itami S, Terashi H Takayusu H. Viability of isolated single hair follicles preserved at 4�C. Dermatol Surg 1999;25:26-9.
[Google Scholar]
|
| 50. |
Raposio E, Cella A, Panarese P, Mantero S, Rolf E, Nordstrom A, et al. Effects of cooling micrografts in hair transplantation surgery. Dermatol Surg 2001;27:98.
[Google Scholar]
|
| 51. |
Saeger D. Chubby vs skinny grafts. Dermatol Surg 1997;23:757-61.
[Google Scholar]
|
| 52. |
Beehner M. A comparison of hair growth between follicular-unit grafts trimmed "skinny" vs. "chubby." Dermatol Surg 1999;9:16.
[Google Scholar]
|
| 53. |
Haddab AM, Kohn T, Sidloi M. Effect of graft size, angle and intergraft distance on dense packing in hair transplants. Dermatol Surg 2004;30;846-56.
[Google Scholar]
|
| 54. |
Meza DP. Complications in hair restoration surgery. Hair Transplant Forum International 2000;10:5.
[Google Scholar]
|
| 55. |
Bernstein RM, Rassman WR. What is delayed growth? Hair Transplant Forum Int 1997;7:22.
[Google Scholar]
|
Fulltext Views
3,540
PDF downloads
1,856





![[Figure - 1]](#fig_ijdvl_2006_72_2_103_25634_1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2006_72_2_103_25634_2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2006_72_2_103_25634_3.jpg){kind=link}
![[Figure - 4]](#fig_ijdvl_2006_72_2_103_25634_4.jpg){kind=link}